 On March 3, 2020, I received the following email from Matt Florey, Cancer Control Strategic Partnerships Manager, American Cancer Society:
“Mr. Desjarlait: Congratulations! Yesterday, a panel representing 6 different organizations reviewed nominations for Minnesota Colorectal Cancer champion of the year. The group unanimously voted to recognize your efforts to increase cancer screening. We will be publicly announcing this award as part of the program at the MN Blue Reception on Thursday, March 12th from 6-7:30 pm at the Como Zoo and Conservatory in Saint Paul.” I was surprised by the announcement. I knew that people were often recognized for their work in Cancerland. But I never expected that my work as an advocate in the Native community would be recognized. Natives didn’t get much play in the mainstream cancer world. But, then, that was, to me, the significance of the award. It wasn’t about personal recognition, but rather recognition that the Native community was part of the equation in the relentless battle against cancer. But then there was the pandemic. On the day before Governor Walz issued his first Emergency Executive Order, the event was postponed. Mr. Florey’s email stated: “Please stay tuned for the official announcement.” My assumption was that the event would be rescheduled at a later date. Days, weeks, months went by. During that time. I didn’t receive any word on rescheduling the event. Was it forgotten? On October 28, 2020, I decided to send an email to Mr. Florey inquiring about the award. He responded: “I am sorry we didn’t follow up more clearly. The framed certificate is in my office but I would like to find a way to share that award on a stage. I am going to reach out to my colleagues to see if we could schedule a web presentation that might work for your schedule. That would allow us to invite others and potentially record it.” It looked like things were finally rolling. I had expected a response within a few weeks as to what the plan would be. But I didn’t get a response. On December 18, 2020, seven weeks later, I sent an email to Mr. Florey asking what was going on with the award. He responded: “My apologies. I should have gotten back to you. We are planning to recognize you and other awardees from 2020 on a webinar in 2021. In early January I will send out a couple of potential dates and times to see if there are any that work better for you.” A few weeks went by and I heard nothing regarding the award. On January 26, 2020, I wrote a post on Facebook regarding Mr. Florey’s mishandling of the situation. I concluded by writing: “I’m not sure what the holdup is. In the age of Zoom, hosting an event shouldn’t be a problem. I’ve pulled a fairly heavy load as a survivor speaking about cancer, writing about cancer, and living as a survivor. “Our stories as survivors are important because we give hope to others. We refuse to be mere statistics used for graphs or for fund-raising. And, it’s important that Native American survivors receive recognition. All too often, our struggles, and stories, get lost in the mainstream cancer world. “But, getting shoved in the backroom is an old story for us. It’s been going on since 1492. A new day doesn’t bring change. It’s just a repeat of yesterday.” Mr. Florey responded later that day: “My apologies for not contacting you sooner and for any hard feelings I may have caused. I should have followed up with you sooner to confirm our plans for your recognition in March of 2021. “In past years we asked for award nominations in January for the previous year but in 2021 it is our intention to honor those that would have been recognized in 2020. We would like to recognize you if you are still interested in participating. I plan to reprint the certificate and retrieve the frame that has been in my office since March of 2020.” On March 3, 2021, I sent an email to see if the award had been sent out. Mr. Florey’s response was: “I will double check and follow-up with you.” There was no “follow-up” by Mr. Florey. Instead, I followed up with an email on March 20, 2021 and asked about the award. Mr. Florey wrote: “I am sorry it has not arrived. I will follow-up with the colleague who agreed to mail it (she has been on vacation) and I will make sure we get something else in the mail (with a tracking number) if I do not hear from her today. My apologies for the delay and thank you again for your distinguished service. Best wishes.” On March 22, 2021, Mr. Florey sent an email verifying the Zoom award presentation (on March 23) and ended his correspondence with: “Could you send me a mailing address so that we can send you your award?” I thought it was a bit odd that he was asking for my address after an exchange of previous emails in which I was told the award was going to be mailed. Despite that, I thought that now that he had my address, the award would be in the mail and I could expect it in a week or two. But, a week or two turned into two months. On May 22, 2021, I sent an email to Mr. Florey and, once again, asked about the award. But this time there is a change-up. Two months later, there hasn’t been a response. Apparently to Mr. Florey, who represents the American Cancer Society in this matter, out of sight, out of mind is the best way to handle the situation. For me, although I received the 2021 Minnesota Colorectal Cancer Champion of the Year recognition at the Zoom event, I have yet to receive the actual award. Call it being in a canoe without a paddle.
0 Comments
 On Friday (Jan. 29, 2021), I go in for my six month check up that includes lab/blood work and CT scan. This will be my 18th CT scan since I first contracted colon cancer in 2013. Fourteen of those scans have happened since 2017 after recurrence (November 2016) that resulted in a five-year high-surveillance program that included scans every three months for three years and scans every six months for two years. I’m now in my last year. According to my timeline, I should reach the five-year benchmark this summer. Assuming that I remain NED until then, my oncologist will declare me as "cancer free." But the cancer journey doesn’t end there. Continued surveillance treatment will most likely include annual lab/blood work - for years. And there’s the reality that one in six cancer survivors develop a second cancer. This isn’t the same as recurrence; rather, it’s developing a wholly new cancer in one’s body. Then, there’s all those CT scans. CT scans use X-rays, which are a type of radiation called ionizing radiation. It can damage the DNA in your cells and raise the chance that they'll turn cancerous. In normal circumstances, having a few CT scans shouldn’t be a problem. But having as many as I’ve had raises my concern. So, I’ll never really be "cancer free." There’s the trauma and associated PTSD of surviving cancer twice and, in particular, the chemotherapy and side effects that I went through. Although chemo has had a significant role in overcoming cancer, some side effects remain today. Additionally, I've been immunocompromised as a result of chemo and leaves me in potentially dire straits should I contract Covid-19. The fear of The Beast lurking in some dark corner in my body is, to me, part of being "cancer free." This disease doesn't let you go scot free. However, one doesn’t have to live a fearful life. Survivors survive because they sing the stories of their healing. My healing song includes my art and my writing. I have goals before me. I may not achieve all my goals, but the importance is doing what I can. Because the effort itself is part of healing from the trauma. My Anishinaabeg ancestors considered sleep to be akin to a state of death. Dreams were a portal to the Unseen World. With the dawn, one's life was renewed. One offered asemaa (tobacco) to Gichi-Manidoo (the Creator) for giving life back. Then, one set out to accomplish their goals for the day. I rely on traditional beliefs as part of my journey as a survivor. Our lives are renewed each day when we awake. We put out our offering and set out to accomplish to goals that we've placed before us. Most importantly, we shouldn't overburden ourselves with goals but keep them short term and accomplishable. Our future is what lies in the day ahead. As such, the shadow of fear is lessened on our journey as survivors. Hope is what guides us, not fear. We need not worry if we leave an unfinished garden. It's what we've planted that give hope and courage to others. © 2021, Robert DesJarlait
"One day, the Earth was submerged by a destructive flood sent by Mishibijiw, the Great Underwater Serpent. Nenabozho, our Great Uncle, survived. Drifting on a log, he obtained pebbles of dirt from the muskrat. After planting the dirt on his log, the Earth regrew and new life reemerged from the life that existed before.” In April 2013, I heard the three words that you don’t want to hear -–“you have cancer.” I thought my life was over. I was 66 years old, retired, and at that point in my life, art was far from my mind. One day, I took a walk in the halls of the cancer ward with my IV stand rolling beside me. My prognosis was good. Following surgery for the removal of my ascending colon, my cancer was classified as Stage I meaning the cancer hadn’t metastasized and chemo wasn’t required. As I walked along the hallways of the cancer ward, I saw walls covered in art. I had no idea who the artists were. I asked a nurse: “Who are the artists?” She replied that some of them were by former cancer patients and other works were gifts from families who had lost a loved one to the disease. And, therein, a seed was sown and a promise made that someday I would return with a painting to join the walls of art in the cancer ward. But any aspirations of returning to art came to a jolting halt in May 2016. My annual CT scan revealed a lesion on the left lobe of my liver. This time around, my surgery was preceded by four rounds of neoadjuvant chemo and followed by twelve rounds of adjuvant chemo. As a result of my recurrence, I became a Stage IV(A) cancer survivor. In November 2018, I decided to try to engage in fine art as part of my cancer journey. Cancer survivors live a cautiously optimistic life. We really can’t look too far into the future. Goals and priorities need to be in the short term. The ideas that floated through my mind in the cancer ward slowly came to fruition. But it was really a question of whether I could return, or more specifically reemerge, to the fine art form I established as an artist in the 1980s. “Gidagaabinesh” (Spotted Bird) was the first work and a tribute to Herb Sam, one of my spiritual mentors and advisors who passed from liver cancer in September 2018. I didn’t have watercolors or brushes, so I decided to use colored pencils and, for the first time, watercolor pencils. I decided to do the work encompassed in a circle - the circle was a hallmark of my illustration art in the 1990s and early 2000s. “Gidagaabinesh” was a test of sorts. Did I retain my skills as a fine artist after a nearly 35 year absence? Or had my abilities diminished? With the finished work, I found that my palette hadn’t lessened and my aesthetics had matured. Indeed, rather than being diminished, they had improved. It was almost as if they had been in limbo and waited for the reopening of the channels to my creativity. I did a sister piece - “Aazha miinawaa Manidoo-Giizhikens” (Aazha and the Spirit Tree) with two main characters from a children’s book I’m writing about two Ojibwe children with childhood cancers. Manidoo-Giizhikens has a special place in my heart following a photo shoot there in 2016 with well-known photographer Ivy Vainio. After completing the two works, I decided to create a body of work called Reemergence. From late November to late January, I worked on a number of pencil studies that would form the series. The art largely reflected the themes I developed in the 1980s – scenes of the traditional, everyday roles of Ojibwe-Anishinaabe women and men. In mid-March, I obtained watercolors, gouache (a new medium for me), and brushes, and began working on the paintings. By mid-June, I completed 15 paintings for a total of 17 works for the Reemergence series. The title reflects my reemergence as a fine artist. But it also reflects my reemergence after battling cancer for seven years. Reemergence is not cancer art per se; rather, it’s art by a cancer survivor who is Ojibwe-Anishinaabe who is an artist. The art is a paradigm of creativity and healing in a time of sickness. However, Reemergence has a deeper meaning. In a cultural context, Nenabozho’s story has a metaphorical meaning in relation to my cancer experience. Cancer and Mishibijiw are interrelated as malevolent beings that bring death, chaos, and destruction. The log is my physical body and Nenabozho represents my spirit. The pebbles of dirt are the medicines that help heal me. And, forthwith, a new life reemerges from the life that existed before. Our elders teach that our personal lives move in a circle. We always come back to a point that we’ve left behind. We may bypass the point and move on. Or we may stop at the point and find something that provides a deeper meaning and direction on our path. With Reemergence, I’ve reached such a point.  Wiizhaandige Gitigaan (Unfinished Garden): A self-portrait of my cancer journey © 2019, Robert DesJarlait
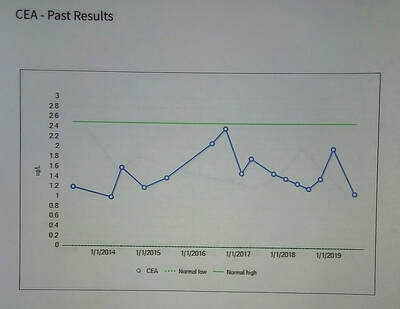 I finally received the results of my CEA results from my lab/blood work and CT scan from July 15. (For the record, I was NED.) (Also for the record, all my lab/blood work came out within the ranges.) CEA stands for carcinoembryonic antigen. The CEA test measures the amount of CEA in the blood, and sometimes in other body fluids. CEA is a type of tumor marker. Tumor markers are substances made by cancer cells or by normal cells in response to cancer in the body. A CEA test can't tell you what kind of cancer you have, or even whether you have cancer. So the test is not used for cancer screening or diagnosis. But if you've already been diagnosed with cancer, a CEA test can help monitor the effectiveness of your treatment and/or help find out if the disease has spread to other parts of your body (CEA information from MedicinePlus). In my case, I've had 16 CEA tests since May 2013. Put another way, I've had 16 CT scans since I was first diagnosed with cancer in 2013 to July 2019. That's a lot of CT scans but it gives you an idea of what a high-risk, high-surveillance patient goes through. Initially, I was Stage I; with recurrence in May 2016, I became Stage IV. I still have 2 1/2 years remaining for CT scans or, according to the math, five more CT scans remaining for my five-year high-surveillance program. Initially, I was on the five-year program but in the third year recurrence happened and I had to start all over again with CT scans every three months for two years and then scans twice a year for three years. The normal range for CEA is 0-2.5 ug/L. CEA usually doesn’t enter the equation until one has been through surgery and is in treatment (chemo/radiation) or prior to treatment. High levels of CEA could or may indicate the presence of cancer or recurrence. Normal levels following treatment indicate that the cancer was likely all removed. But back to my CEA tests. My first CEA test on May 1, 2013 was 1.1 ug/L. Given the fact that I had a tumor the size of a lime in my ascending colon, the low CEA reading is remarkable. In short, it appears that my CEA wasn’t a determinate factor in evaluating the presence of cancer. In the four CEA tests that followed over a two year period, my CEA was 1.0, 1.6, 1.2, 1.4 respectively. Then there was a slight spike at the time that my recurrence was diagnosed. In late May 2016, the level was 2.1. Right before my recurrence surgery in November 2016, the level was 2.4. I had my first post-surgery CT scan in January 2017. The CEA level was 1.5. There was a slight spike in April 2017 - 1.8. Then, in the following 2 years the levels were 1.5, 1.4, 1.3, 1.2, and 1.4. In January, the CEA spiked to 2.0. In July 2019 (my most current CT scan/CEA test), the CEA level was 1.1. I think what is interesting is that at the time of my recurrence and the two spikes in my CEA in association with it, the levels were still in the normal range. Was it because the small size of the lesion on the left lobe of my liver? The 2.4 reading before my recurrence surgery was high but still within the threshold of the normal range. Perhaps, in some cases, the CEA doesn’t have to spike over the threshold to indicate the possibility of cancer. Usually, when I read my CEA results, I’m looking for higher numbers - 3.0 or beyond. CEA is a hot topic in the cancer support groups that I’m a part of. I’ve seen people with 5.0 to 8.0 CEA levels. High numbers like that is a cause for alarm. But, again, perhaps the numbers don’t have to be that high for some survivors. With that said, the spike to 2.0 in January 2019 is a bit worrisome. It jumped from 1.4 to 2.0. Why the spike? Certainly, my current level of 1.1 provides some solace. But in the back of my mind is always the thought that cancer cells are floating somewhere in my blood stream patiently waiting to take foothold somewhere. And, perhaps, that quirky, recent spike may be telling me something. Hopefully, it isn't.  “As a Stage IV cancer survivor, reengaging in my art provides a path for healing and has allowed me to return to my roots as a fine artist." Reemergence: Returning to the Circle
July 19 to September 6, 2019 Two Rivers Gallery 1530 E. Franklin Ave. Minneapolis, MN 55404 Robert DesJarlait will exhibit his new series “Reemergence” at Two Rivers Galley located at the Minneapolis American Indian Center. The solo exhibition features 17 new works in mixed watercolor mediums. The exhibit opens on July 19, 6-8 p.m. This is DesJarlait’s first solo exhibition since 1990. In subsequent years, he established a career as an illustrator for Native American organizations and school programs and as a muralist. “Reemergence” marks his return to fine art. In 2013, DesJarlait contracted colon cancer followed by surgery. In 2016, he went through surgery again for recurrence of cancer. “As a Stage IV cancer survivor, reengaging in my art provides a path for healing and has allowed me to return to my roots as a fine artist. The themes and stories of traditional lifestyles and activities that dominated my art in the 1980s are retold from a fresh perspective of a renewal of life. My Reemergence Series is a testament of resiliency in facing the Asabikeshiinh (Spider) within.” DesJarlait is from the Red Lake Ojibwe Nation and currently lives at Onamia, MN. Contact Information: Telephone: 218-380-8491 Email Address: [email protected]  In Cancerland, we often employ terms that help us define our situation in dealing with this disease. Such terms gives us a sense of focus, balance, and hope. The most used term is “cancer warrior.” By employing combat/military terminology, we see ourselves as battling a fierce foe - one that is cunning, baffling, powerful.
Of course, we’re not alone in this battle. We have cancer teams composed of oncologists, surgeons, and nurses. And we are provided with weapons to engage the enemy- surgery, chemotherapy, radiation, immunotherapy, and personalized medicine. Another weapon is our spirit - one in which spirituality and/or faith play a central and powerful role. Spirit is, I think, the underlying force of identifying and defining oneself as a cancer warrior. In this sense, our bodies are a battlefield. We go through surgery. We go through treatment. The effects of that battle leave indelible scars on our bodies, and treatment leaves long-lingering after-effects and PTSD. We’ve survived cancer but it’s with a future that is uncertain. As cancer veterans, we live a life in which we are cautiously optimistic. In any battle, the objective is to beat the enemy. But beating the enemy doesn’t necessarily mean annihilation of the enemy. It means eradicating the enemy from the present battlefield. The enemy has retreated but lurks elsewhere. Even after cancer surgery, it’s estimated that over a billion cancer cells continue to circulate in the body. So, the cancer is never really gone. It doesn’t mean that The Beast will come back. But the opportunity is there and cancer is all too often an opportunist. Given the right conditions, cells can gain a foothold on another organ and metastasize into a deadly colony. I have first-hand knowledge of this when rogue cells invaded the left lobe of my liver, thus commencing my second battle with The Beast via recurrence. At this point, it appears that I’ve “won” my second battle with cancer. But the war is far from over. I still have three years on my high-risk surveillance program- three years of semi-annual CT scans with lab/blood work and annual colonoscopies. And that brings me to why I decided to write this article. Quite often when I write something, it’s a response to something I’ve read. Such is the case with “The Problem With The Phrase 'Beat Cancer'” by Brittany Wong. Wong writes about telling her now deceased father, a Stage IV terminal pancreatic cancer patient, that he could beat cancer. Of course, there wasn’t any way her father could beat cancer at that stage of his illness - he was at the end of his journey. In retrospect, Wong writes: “The idea that you can “beat” something as insidious as cancer perpetuates the myth that the patient is wholly responsible for their recovery, not a human caught up in an endless cycle of surgeries, chemotherapy, radiation and relapses. And if they don’t beat it? That’s failure.” Wong’s article is yet another part of a larger conversation regarding the use of combat/military metaphors in Cancerland. In this case, telling a terminal metastatic patient that they can beat cancer implies there is hope in overcoming cancer at a point when it is incurable. At that point, there really isn’t any hope. There is no longer a fight or battle. With Stage IV advanced cancer that is terminal, one cannot conquer death. Stage IV cancer isn’t necessarily an immediate death sentence. Stage IV is defined as advanced or metastatic cancer. Some people may be initially diagnosed with Stage IV cancer. They already have incurable cancer that has spread through their body. Depending on the type of advanced/metastatic cancer, a patient undergoing chemo or radiation may live for several days, months, or even for a few years. Treatment doesn’t cure their disease, rather it extends their survival. Newer therapies like immunotherapy work in combination with chemo and/or radiation to extend life. However, immunotherapy is only available for certain individuals with certain types of cancer. And immunotherapy may or may not work. Some individuals may progress into Stage IV from their previous stage(s) of cancer. In my case, in 2016, I went from Stage I to Stage IV as a result of recurrence to my liver. Fortunately, my recurrence was limited to the left lobe of my liver. Technically, my cancer was oligometastatic meaning a single metastases had occurred to my liver. Oligometastatic is defined as a single or only a few metastases to an organ. My oligometastatic cancer was treated with metastasectomy surgery to the left lobe of my liver where the metastases had occurred. Treatment included neoadjuvant and adjuvant chemo followed by a 5-year high-risk surveillance program. What is unusual about my metastases is it occurred three years after my surgery for Stage I colon cancer. Unusual, yes, unique, no. The 5-year survival rate for Stage I colon cancer is 93%. Which means that 7% of survivors can develop metastases that can, in time, be fatal, or could be potentially curable if the metastases is caught early and treated with a metastasectomy and chemo and/or radiation. At this point, I have been a survivor for 5.8 years with a Stage IV survivorship of 2.7 years. As a 5+ years as a cancer survivor, I’m a realist. Even if I reach the 5-year survival mark that technically makes me cancer “free,” I don’t think I’ll ever say that I beat cancer. There are too many intangibles involved that prevent a total victory in becoming cancer free. I can, however, say that I’ve beat cancer another way. Aside from doctors and medical procedures, the only thing I’m really bringing to this battle is my spirit. And, that’s one thing that cancer will never beat. I realize that ultimately cancer could beat me. But it won’t beat my spirit. And, I think, that’s what beating cancer is about. Certainly, it’s about overcoming the medical obstacles, but it’s also about one’s strength of spirit. Perceiving myself as a cancer warrior and using associated metaphors doesn’t give me a sense of false hope. I know what my odds are. Perhaps more importantly, being a cancer warrior gives hope and courage to others who may, at some point, engage this disease or those who are already engaged with cancer. Being a cancer warrior is about the strength of spirit and soul in facing fierce foe. We are the storm.  “Robert, you’ve had some second chances,” my cardiologist said, “You might be pushing things.” The conversation came near the end of my annual visit with my heart doctor. Two days prior to my visit, I had my quarterly lab and CT scan that are part of my high-risk cancer surveillance program. The CT scan came out as NED – “No findings to suggest local recurrence or metastatic disease in the chest, abdomen, or pelvis.” In the words of my oncologist, my scan and lab/blood work came out “great.” My heart doc went back over the results and noted specific areas that pertained to my heart. The only areas of concern were my two aneurysms - a thoracic aorta aneurysm which was stable and unchanged, and an abdominal aorta aneurysm in which there was a mild dilatation. Both will require stents at some future point, but, for now, they are not areas of concern. Other than that, my heart doc said my heart was in good shape with excellent results regarding my lipids and cholesterol. The conversation then turned to my high blood pressure problem. In my last three CT scans, my BP was high - 146/85 (1/21/19), 148/85 (10/16/18) and a whopping 151/80 (7/16/18). My BP that morning at the heart doctor was 106/72. Needless to say, I had my concerns. Although my heart and blood work was fine, I didn’t like the idea of being visited by a sudden stroke. “Do you still smoke?” he asked. “Yes,” I answered. “I smoke about 7-8 cigarettes a day.” It was no secret to my cancer team that I smoked. It was on my medical profile. At the time of my heart attack in November 2012, I was smoking nearly two packs a day. “Robert, you’ve had some second chances. You might be pushing things. Seven or eight cigarettes are still too much. Right now, you’re free of cancer. So, there’s that. And your blood pressure problem could be very well related to your smoking. It’s time you quit.” At this point, readers may wonder why in the world a cancer patient would smoke. You would think that two cancer surgeries and sixteen rounds of chemo would be enough to quit. Some people never get a second chance. So why double-down and flirt with The Beast? Smoking among cancer patients/survivors is one of those “inconvenient truths.” I observe that disturbing truth when I go for my appointments at the cancer hospital. Patients in their gowns, arms attached to IV stands, hunched over and smoking in designated areas outside the hospital. It doesn’t matter if it's raining, snowing, or cold. They are always out there. Walking contradictions lost in the plumes of smoke. And I was part of that inconvenient truth with my habit of 7-8 cigarettes a day. According to the Surgeon General’s report in 2014:
It’s estimated that about half of patients who smoked before their diagnosis continue to smoke following cancer treatment, and that many who quit relapse. “With the stress cancer patients are under, they tend to be at higher risk of relapsing for a longer period of time,” said Brian Hitsman, associate professor of preventive medicine at Northwestern University Feinberg School of Medicine. “Personally, I’m not surprised,” said lead researcher Robert Schnoll, a psychologist at University of Pennsylvania. “I’ve been working in nicotine dependence research for 20 years. The brain chemistry is affected by decades of exposure to nicotine. Some patients view [smoking] as critical to managing the stress in their lives.” Depression is another factor. Approximately 58% of cancer patients suffer from depression compared to 10% of the population. For me, aside from addiction, stress and anxiety are significant factors. It’s not easy being a cancer survivor. I don’t sit around and constantly think about a recurrence that will come back and kill me. But I think just living with cancer, despite bring NED, is in and of itself a stressor. It seems like I’m living from CT scan to CT scan and not knowing what the next one will bring. And the scanxiety is more acute on the day of the scan. And there’s the stress of everyday life of a survivor. Little aches and pains that become magnified and with it the thought - has it come back? In 2012, following my emergency angioplasty, I began using an electronic cigarette. That seemed to work although the strength of the nicotine was basically the same as a nicotine patch. The attraction of the e-cig was it was similar to a smoking cigarette - a long, thin object shaped like a cigarette that you placed in your mouth, inhaled, and exhaled smoke. Four months later, I was diagnosed with colon cancer. My oncologist gave me a prescription for nicotine patches and an inhaler. But those didn’t work and I began smoking 1-3 cigarettes a day. Eventually, I worked my way to my current level of 7-8 cigarettes a day. Of course, I’ve always felt guilt and shame by smoking. Cancer survivors, of all people, should know better than to smoke. And I think that those of us who do continue to smoke feel like pariahs in Cancerland. However, according to Dr. Alberg, Professor of Public Health Sciences and the Associate Director of the Hollings Cancer Center in South Carolina: “So, I think first and foremost, please recognize that smoking cigarettes is not a failing of you as an individual. If you are a smoker, it is not a personal failing. Most adult smokers tried cigarettes when they were young, in childhood or when they were a teenager, usually for social reasons, and from that experimentation, end up with a nicotine addiction that can be very difficult to overcome. So recognize that this is an addiction, that it's not easy to overcome, but can be overcome with effort and with the appropriate help.” Dr. Alberg’s words don’t give us the green light to smoke. Rather, his words help us understand that our addiction is deep-rooted and, perhaps more importantly, we’re not failures (or pariahs) because we continue to smoke. Looking back, I can say I had appropriate help. My oncologist, assistant oncologist and nurses encouraged me to quit. Nicotine patches were offered and brochures for QUITPLAN were given to me. My cancer team thought it was a bit of an achievement to go from two-packs a day to under a half pack. But they felt that I should take it a step further and quilt altogether. What was lacking was any real effort on my part. Smoking cessation products can help curb the need for nicotine, but cessation requires the will to quit. And having the will to quit is the most difficult part of cessation. It was my cardiologist who gave me the sternest lecture on the hazards of smoking. He wasn’t talking about the effect of smoking on my heart since my heart was in good shape. Rather, he emphasized the danger of contracting a secondary cancer. We decided on a prescription for Chantix. Oddly, I had never been offered such a prescription from my oncologist. Perhaps such a prescription had to come with my heart doctor’s approval since Chantix’s side effects could impact my heart. My heart doc said that Chantix wouldn't interfere with my current heart regimen of metoprolol, lisinopril, baby aspirin, and rosuvastatin. And because I was in good shape physically, including my heart, my heart doctor green-lighted the prescription for Chantix. Of course, I realize that all this time I’ve only been kidding myself. Seven to eight cigarettes may sound good compared to two packs. But that doesn’t make me immune from secondary cancers. And contracting secondary cancers runs high in survivors who smoke. And then there is my high-risk cancer surveillance program that is scheduled to run for over several years with periodic CT scans and lab/blood work. I admit that I’ve harbored the thought that if any recurrence or secondary cancers develop, the scans will catch it in time, so why worry about a few daily cigarettes? But do I really want to face the consequences of that route? Face the possibility of more surgery and chemo? Or what if The Beast metastasizes so quickly that it can’t be stopped? I had a dream about this the other night. I was holding a box of Chantix. I was looking at a pill. My finger was over the plastic bubble and slightly applying pressure against it to pop it out. In the shadows, The Beast gleefully lurked and encouraged me to stay my hand from popping out a pill. As of this writing, I have yet to begin my smoking cessation program. But the dream gave me an obvious choice of what I need to do. It isn’t just about quitting smoking. It’s more about preventing the deadly specter of The Beast back into my life. In Cancerland, The Beast (or whatever you chose to call it) is always the foe. That’s what the battle is all about. Second chances is about not relinquishing to the enemy. And second chances is about reaching and maintaining a quality of life in which one can achieve personal goals. Not everyone has the opportunity for second chances. I do. © 2019, Robert DesJarlait
 Whenever I’ve spoken about cancer, I’ve often done so with a measure of pessimism. Why so? Consider my cancer history. Colon surgery in 2013 with a classification of Stage I. My future looked rosy and bright. After all, Stage I has a 5-year survival rate of 93%. I only had to reach the 5-year benchmark and could then consider myself cancer free. It seemed simple enough. Chemo wasn’t required and I only had to have annual CT scans for five years for my treatment regimen. Following my second CT scan, it became routine. I was NED and I assumed that I would continue as NED until I reached the 5-year mark. But in my third year, 2016, I fell into that 7% survivor gap as a result of a cancerous lesion found on the left lobe of my liver. What had been simple and routine turned into a cancer survivor’s worst fear. I spent 9 hours in OR - three hours for the removal of the lobe and 6 hours for an incisional hernia (that was a result of my surgery in 2013) ; and went through 16 rounds of chemo with all its attendant side-effects. And I moved from Stage I into the Stage IV category. Along with all that, I was put on a high-risk surveillance program consisting of CT scans every three months for two years followed by CT scans every six months for three years. I’m about to complete the two-year portion with the three-year program still ahead of me. As of this writing, I’ve been NED for 2 years, 1 month, and 28 days. It’s little wonder why I’ve often said that cancer will probably end up killing me. However, that doesn’t mean I’m pessimistic and filled with doom and gloom. My life is filtered with strong rays of hope guided by a core of spirituality. There are still things for me to accomplish in the days and months ahead. The key is not to set my priorities too high and set goals that I feel I can accomplish within reason. Of course, I don’t want people to read too much pessimism in my outlook. After all, I am a cancer advocate and activist. However, I've found that my outlook is one that is shared by many other survivors. In our commonality, we go through the pangs of scanxiety whenever our next CT scan is due. We literally hold our breaths while we await the results from our onc. Then there is the lab/blood work that accompanies the scans. Will our CBC w/ Platelets Differential be within the normal ranges? And will our Comprehensive Metabolic Panel be at acceptable levels? Is our CEA level too high or too low? This is what life is like for a survivor. Is it any wonder why I might be a bit pessimistic? But hope fills in all those gaps created by my limited pessimism. I know it probably sounds like an oxymoron to say you’re pessimistic yet optimistic. However, an introvert can be an extrovert at times. There’s a difference in living with a doom and gloom mindset and living outside it. Living outside it means to attain a quality of life and move ahead to accomplish goals. And it is the light of hope that guides us. There will always be those nagging doubts. Yet, we have much to look forward to. Call it being cautiously optimistic. © Robert DesJarlait, 2019
 Video Link: The Powwow Colon Cancer Initiative was a special project sponsored by the American Indian Cancer Foundation with a grant from the Minnesota Department of Health. I was asked to be the spokesperson for the project. From April to June 2018, we attended six powwows - the Osseo Indian Education Powwow, Augsburg Powwow, University of Minnesota Powwow, Leech Lake Memorial Day Powwow, White Earth Annual Powwow, and the Lake Vermilion Powwow. The powwows gave me the opportunity to talk about my survivor story and to provide information on colon cancer. The most important message was, and is, that colon cancer is preventable. Cancer is a word that is a stigma for some people – Native and non-Native alike. Some people feel that it shouldn’t be spoken. By not saying it, the thinking goes that you won’t get it. But by not talking about it, we deny its existence. Denial can be deadly because denial can prevent a person to seek screening. Denial allows for cancer cells to grow and multiply and advance from a treatable Stage I cancer to a deadly Stage IV cancer. In my initial contraction of colon cancer in 2013, a tumor was found and my ascending colon was removed. It was classified as Stage I because the cancer hadn’t broken through the walls of my colon. Survival rates for Stage I are great. However, in 2016, a cancerous lesion was found on the left lobe of my liver. The lobe was removed and I went through 16 rounds of chemotherapy. I have remained cancer-free for two years. Because of my recurrence, I am considered as a Stage IV survivor. In hindsight, all of this could have been avoided had I gone to my doctor for colon cancer screening at the recommended age. But because I didn’t, a pre-cancerous polyp developed into a adenocarcinoma (cancerous) polyp with mutated cells that multiplied into large tumor. It takes 7-10 years for a pre-cancerous polyp to develop into cancer. Had I gone in for screening, I wouldn’t be writing this nor appear in a video. Had I gone in for screening, I wouldn’t be dealing with post-chemo after-effects, effects that can potentially linger for many years. The Powwow Initiative video marks an important place on my cancer journey. Since 2013, I’ve served in the role of a cancer advocate in the Native American community. The video is a visual representation of the message that I carry. It’s a simple message but one that can save lives. Please share my message with others. Together, we can help prevent this second cause of cancer death among Native people. Miigwech to videographer Tiana LaPointe, Kristine Sorensen and In Progress, the American Indian Cancer Foundation, and the Minnesota Department of Health. |

Robert Desjarlait
|


 RSS Feed
RSS Feed
