|
I’m tired. I’m weary. When I say I’m weary, I don’t mean physically. I’m weary emotionally and spiritually. It isn’t a constant weariness. It comes and goes. It comes especially when I receive news of someone I know who has contracted cancer. This past summer alone, I personally know of six people who have contracted cancer. These are close and dear friends, people who are known in our community. These are people who have been newly diagnosed. In some cases, the cancer is untreatable and, hence, terminal. In addition to that, several people I know are batting recurrence through treatment. And then there are the people I don’t know personally but know through Facebook. People who have contracted cancer, people who have died from cancer, and people who have lost loved ones to cancer. Why all this cancer in our community? I don’t know. However, I’m not really thinking about the reasons for the rates of cancer among my friends. I’m thinking about those who are getting this horrid disease. It’s unending. And I may be more attuned to this depressing news because I’m always writing about it. It brings up the question - why them, not me? I don’t know. Perhaps I’m here to tell the story. Is it normal to feel this way? I thought maybe it was just me. But then I went online and found several articles on cancer survivor’s guilt. As it turns out, the way I feel at times like this is fairly common among cancer survivors. And the feeling is - some have survived, others haven’t. With it there can be a sense of guilt. I’ve survived, you haven’t. I don’t say that with any pride or self-indulgence. Rather I say it with tears and sadness. Survivor’s guilt is part of the psychological effects that impact survivors. Those effects include fear of relapse or death, chronic anxiety, uncertain future, fear of dependency, PTSD or depression, and survivor’s guilt. People, including caregivers, are generally unaware of the inner feelings that survivors deal with. If a loved one is surviving cancer and living in partial or complete remission, then they assume that the person is okay. But they don’t really see what’s under the surface. And that’s why being a survivor is a private, and oftentimes, isolated experience. You can’t know what it’s like being a survivor unless you are a survivor. Certainly, those psychological impacts are part of the reason why I write and talk about cancer. In turn, I have my critics. Some people, especially elders, have told me that I shouldn’t talk about cancer. For them, the word is a stigma. Apparently, if you don’t talk about it you won’t get cancer. Then there are others who have told me to “get over it.” Get over what? Get over cancer? I wish I could. But I’m stuck with it for the rest of my life. And, for me at least, this is where a few of those psychological factors come into play, especially fear of relapse and uncertain future. My cancer, or more specifically my recurrence cancer, has been in complete remission for over 18 months. That doesn’t mean that I’ve been cured of cancer. Only when I’ve been in complete remission for five years can I be considered to be cancer free. I still have 3 1/2½ years to reach that goal line. And, as defined by the American Cancer Society, “A complete response or complete remission does not mean the cancer has been cured, only that it can no longer be seen on tests.” The notion that cancer unseen but lurking in my body creates the thought that it could return. Maybe not today but what of tomorrow? That’s not to say that I live in fear. But I’m not fearless. Perhaps the best way I can put it is that I have a fearful respect toward my cancer. As Augustus Waters says in The Fault in Our Stars: “And what is my cancer? My cancer is me. The tumors are made of me. They're made of me as surely as my brain and my heart is made of me.” I can’t say that I’m not subject to psychological factors. I am. But I’m not overwhelmed by them. Just as cancer is a part of me, so too the psychological factors. Survivor’s guilt is probably the one I deal with the most. But then, that is the factor that I’m most exposed to because of the news I receive on social media. And what strikes me the deepest are friends who are diagnosed with late Stage IV terminal cancer. In the blink of an eye, their world has changed in which there is no tomorrow. They haven’t the opportunity to become survivors. As Augustus Waters says, cancer is a civil war with a predetermined winner. For some, the civil war is lost before even stepping onto the field of battle. Of course, life goes on. I have to continue what I do and live the life I have. And tell the story. © Robert DesJarlait, 2018
2 Comments
Stories are told in different ways. Some stories are told by words that are written or spoken. Other stories are told through pictures. Some stories are told with both words and pictures. Cell phones have, of course, changed the way we tell stories through the photographs we take. The Kodak moment has become the smart phone moment. We no longer have to carry the extra baggage of a camera with accessories. Rather, we carry our camera in our pocket. When we buy a smart phone, we more often than not do so for a camera that allows us to take good, quality photographs that document our personal lives and our relationships with others. On the internet and social media, we download our photos and post them with text. We become storytellers by proxy although it is the photos that emphasize our experiences. With that said, I didn’t really photograph my experiences in Cancerland in the beginning. The only photo I remember taking was from my bed in the cancer ward at U of M/Fairview hospital. The view outside my window was the Mississippi River. Riverside Park was across the river. In the summers of my young boyhood, my family picnicked there on Sunday afternoons. We only lived a few blocks away in the Seven Corners area. Although I posted the photo on Facebook with a short narrative, the post and the photo got lost. Hence, the phase of my cancer journey that I call Stage I was largely documented by others, most notably by Ivy Vainio. Ivy is a preeminent photographer whose photos have been featured in exhibitions and articles. She is something like my personal “paparazzo” who has literally taken hundreds of photographs of me. I don’t know why I am one of her favorite photo subjects, but Ivy has essentially photo-documented my life from 2012 to the present-day. Ivy’s photos from 2013-2015 (Stage I), along with several others, document my life albeit my life lived as a cancer survivor. Things may appear normal but under the surface I was going through a healing period. Whether I was at a powwow or in a march, my physical capacity was limited as a result of my colon cancer surgery in May 2013. The second phase of my cancer journey, that I call Stage IV, begin with photographs that I took of my experiences in the deeper world of Cancerland - a world of CT and PET scans, chemotherapy, biopsies - and my reactions of what I was going through. My goal wasn't to photograph everything but enough to leave a record to tell my story. This then is my cancer journey as told through photographs and words. From the moment that it began to the present. However, there is no ending because the cancer path goes ever on. Stage I 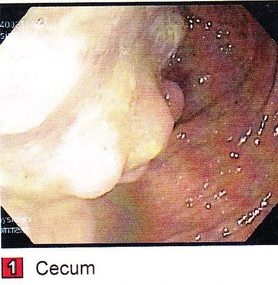 My cancer journey began on 4/26/2013 with a colonoscopy performed by Mohamed A. Hassan, MD, at the University of Minnesota Medical Center, Fairview, Endoscopy Department. The colonoscopy was ordered by Genevieve B. Melton-Meaux, MD, gastroenterologist/surgeon, to whom I was referred to by my doctor, Katherine B. Bickel, CNP, at the Native American Community Clinic. As noted in the colonoscopy report - Impression: Malignant partially obstructing tumor cecum. So began my battle with The Beast. Five days later, I underwent my first CT scan. Examination: CT Chest, Abdomen and Pelvis 5/1/13 Indication: Right-sided colon mass. IMPRESSION 1. Lobulated mass involving the distal cecum and ascending colon consistent with known colon carcinoma. There is intussusception tip cephalad, this is then drawn is a normal, nonobstructive, appendix more cephalad as well. The terminal ileum is somewhat thickened. It may well be that the terminal ileum is thickened because of intermittent intussusception. The size of the mass is likely accentuated due to intussusception. There are multiple lymph nodes in the medial mesentery to a sending colon. The size and number are worrisome for possible metastatic involvement. 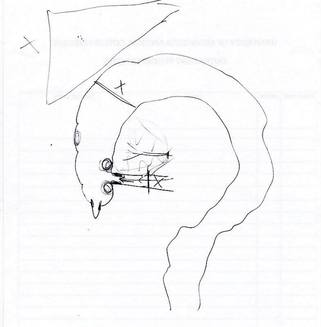 Following my colonoscopy and CT scan, I met with Dr. Melton-Meaux to discuss my surgery. Dr. Melton-Meaux did a drawing of the tumor in my ascending colon. The triangular shape is my liver. She explained that the section of my colon marked by the X would be removed. On 5/14, Dr. Melton-Meaux performed laparoscopic surgery to remove the tumor. My cancer was classified as Stage I. As such, chemo wasn't required. The tumor hadn't broken through the wall of my colon and into my lymph nodes. However, I was put on a high-risk colon cancer surveillance program that included annual colonoscopies and CT scans for five years. I felt that I had dodged a bullet. The five-year survival rate for Stage I colon cancer patients is 93%. I couldn't ask for betters odds. I had beat The Beast in my first battle. My CT scans for 2014 and 2015 reaffirmed the survival stats. I was NED (No Evidence of Disease). Although polyps were found in my post-surgery colonoscopies, none were precancerous (that is, not until 2016). My main concern was an incisional hernia that had developed. However, Dr. Melton-Meaux or Dr. Greeno, my oncologist, didn't feel it was an issue at this point. CT 5/27/14 IMPRESSION 1. Postsurgical changes of a right hemicolectomy with resection of the previously seen cecal mass. No evidence of metastatic disease in the abdomen or pelvis. 5. New incisional hernia containing nondilated loops of small bowel.  Kiwenz Ojibwe Language Camp, 2014 / Photo by Ivy Vainio Following my surgery, my perspective of life and priorities changed. My body, mind, and spirit had been through a traumatic experience. Healing takes time. As part of my healing, I continued to be engaged in various cultural and environmental activities. I began to advocate about cancer in the Native American community. I started a blog to provide insights about Cancerland. Regardless of what I was doing, cancer was part of my renewed persona.   Being a cancer survivor brings many gifts, both material and spiritual. The gifting of my cancer medallion in 2014 was one such gift. The beaded medallion was made by Naakiiyaa Wilson and gifted to me by Ivy Vainio. The ribbon represents the blue ribbon for colon cancer. It encircles a dragonfly, one of my favorite insects.  Photo / Ivy Vainio  Photo / Ivy Vainio  Photo / WCCO News The People's March in November 2014 proved to be a test of my physical stamina. The march was one of two marches held concurrently to protest against the Washington Redskins name and mascot. (The other march was organized by National Coalition Against Racism in Sports and Media.) The People's March was organized by several Twin City grassroots organizations. We brought 1400+ marchers to the streets. I could only make it halfway before handing my eagle staff to my friend Patrick Shannon-Skildum to bring it home to the stadium.  Powwow for Hope, May 2015. Photo / Ivy Vainio My path as a cancer survivor is entwined with the American Indian Cancer Foundation's annual Powwow for Hope (PFH). In 2013, I attended my first PFH. My intention was to dance for my father, Patrick Robert DesJarlait, who died from stomach cancer in 1972. Ironically, by the time that this powwow came up on my calendar, I was dealing with my own cancer.  Photo / Patricia Shepard  Photo / David Goodner Tar Sands Resistance March, June 2015. On a hot, sweltering day in St. Paul, over 5,000 of us marched to the Minnesota State Capitol to bring our message - no more tar sands, no more Enbridge. This was a magnificent march and incredible experience. I only made it halfway with my eagle staff. I handed it off to another individual who brought it to the steps of the capitol.  Manidoo-giizhikens (Little Cedar Spirit Tree), Grand Portage, 2015. Photo / Ivy Vainio. Like many other Anishinaabe people, Manidoo-giizhikens was a tree that I was familiar with through stories and photos. I never expected to see it, let alone stand next to it, touch it, and place asemaa (tobacco) under it. This was undoubtedly an integral part of my healing journey. This is one photograph of several from a photo shoot with Ivy.  Screen capture, NFL Films  Photo / Miziway Migizi DesJarlait Minnesota Vikings Native American Heritage Month celebration, November 2015. A life-long Minnesota Vikings fan couldn't ask for much more than this - dancing before a home crowd of 54,000 at halftime and getting a ringside seat to the Vikings vs. Packers game. The video, shot by NFL Films, has been viewed by over one million online viewers.  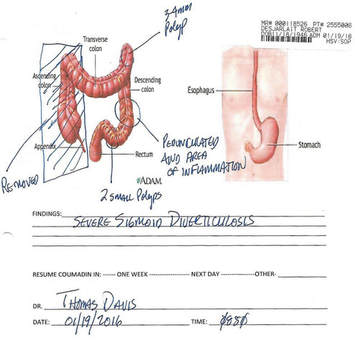 The year 2016 began with a ominous reminder. After a delay of six months, I finally had a colonoscopy performed at the Mille Lacs Health System. Three polyps were found and removed. The 3-4mm polyp in my Traverse colon was confirmed by biopsy to be precancerous. This didn't mean that cancer had developed again in my colon; rather, the precancerous polyp signaled the conditions, in time, for cancer to develop. Of course, it bothered me that cancer, in any shape or form, had been in my body. It raised the question of whether I would ever really be cancer free. Stage IV    On June 23, 2016, I had appointments for lab/blood work, CT scan, and a meeting with my oncologist, Dr. Edward W. Greeno. Because of the early morning appointments, my wife and I stayed at the American Cancer Society Hope Lodge. Little did I know what the day would bring.   After lab work, I did my CT scan. We had to wait two hours before we could see Dr. Greeno and get the results of the scan. The first words that Dr. Greeno said to me was: "Well, Robert, we found something on your scan." I was crestfallen. He explained that a spot was found on the left lobe of my liver. In the photo, my liver is on the left and the left lobe near the top. The dark spot is clearly visible. We were both surprised since we were aware of the outstanding stats for Stage I survival rates. I was no longer Stage I but now Stage IV because cancer cells had traveled through my blood stream and had metastasized to my liver. Dr. Greeno wanted to be sure that the cancer hadn't spread elsewhere, so he ordered a PET scan for the next day. CT 5/23/16 IMPRESSION: 1. New hypodense cystic-appearing lesion in the left hepatic lobe, measuring up to 2.4 cm, most compatible with metastases in this patient with a history of cecal adenocarcinoma.  The PET can confirmed the results of the CT scan - colon cancer mets to my liver. But there was a new concern. A lymph node my neck - the deep cervical lymph node - near the bottom of my neck and collarbone lit up. It would be extremely unusual for cancer cells to travel and metastasize in an area so distant from my cancer's point of origin. But the only way to find out was to perform a biopsy of the lymph node. PET Oncology Whole Body 5/24/16 IMPRESSION: 1. In this patient with a history of cecal adenocarcinoma status post resection, there is hypermetabolism at the periphery of the new hepatic segment 3 lesion, consistent with metastatic disease. 2. Markedly hypermetabolic cervical lymph nodes bilaterally are nonspecific. While this would be atypical for metastatic colon cancer, malignancy cannot be excluded and biopsy should be considered for further evaluation.   A fine needle aspiration biopsy was performed on 6/10. Seven days later I received the results of the biopsy: “salivary gland neoplasm, morphologically consistent with Warthin's Tumor which is a benign cystic tumor of the salivary glands containing abundant lymphocytes and germinal centers.” So, I had a tumor in my neck that was benign with a 3% chance of becoming malignant in 20 years. It was a risky operation. Nerves to the face located next to the lymph node could be severed and cause paralysis of the right side of my face. As a result, it was decided that the Warthin's Tumor would be left alone and not surgically removed.  On the way home from my lymph node biopsy, we stopped at the Relay for Life event at Mora (MN) that I had previously signed up for. I was stressed out, tired, and sore, and not interested in participating in the survivor's walk. I just wanted my survivor t-shirt. We tried to find my luminaria bag but there was simply too many that lined the Mora Fair Grounds. Given the overwhelming number of luminaria, it was obvious that cancer had deeply impacted this small farming community.       In July 2016, I had my first infusion of neoadjuvant chemo. I was scheduled for six rounds of Oxaliplatin via IV and daily tabs of Capecitabine. The chemo was intended to shrink the cancer on my liver. I had a mild reaction to the third round of Oxaliplatin and a severe reaction to the fourth round. As a result, the remaining chemo infusions were cancelled.    It didn't take long for the chemo side effects to take hold. The most immediate was the cold-sensitivity effect. Anything touched by my bare feet and hands resulted in a numbing, tingling sensation. I had to use rubber gloves when using metal utensils and getting things from the refrigerator. I had to drink through straws. My palate changed; some food lost its flavor and other foods were overly intense with flavor. To make up for needed vitamins and minerals, I drank a daily smoothie with fruits and vegetables with Muscle Milk Protein powder. The "What To Eat" book helped me to make more nutritious meals. "The Cancer Survivor's Companion" helped me deal with emotional issues. "Mindfulness-Based Cancer Recovery" enabled me to calm my mind and deal with less stress. I also maintained traditional practices - smudging myself with sage and sweet grass, smoking my pipe, and offering asemaa (tobacco) in the mornings.  In July, I met with Dr. Michele Montejo Loor, MD. By this time, my incisional hernia had grown quite large. The hernia had been noted in previous CT scans and PET scan. Because of its size, it was decided that it would be removed during my liver surgery. I also met with Dr. Eric Jensen, the Surgical Oncologist who would be performing my liver surgery. Surgery was scheduled for November (2016). I would be undergoing two surgeries in one shot - one for the liver and one for the hernia.   In August 2016, a port was inserted for easier access for chemo infusion and for lab/blood work.      Photo / Francisca Wiyakaluta Folkestad  One of the side effects of my chemo was hair loss. I wasn't losing my head hair per se; rather, my hair was coming out in clumps. I also lost my eyelashes. My mustache and goatee remained untouched. On the morning of my port insertion, I had Nan cut off my pony-tail and scalp-lock. The following day, I went to a barber and had my head shaved bald. I kept my pony-tail and scalp-lock, but a week later I took the rest of my hair, made a medicine bundle, and released it on the Mississippi River. A pre-surgery CT scan was performed in October. The cancer was growing albeit slight. The hernia received special attention since it would be part of the surgery that would be performed. CT 10/7/16 IMPRESSION: 1. Slight increased size of left hepatic metastasis. HISTORY: Metastatic colon cancer, assess response to treatment.Malignant neoplasm of colon, unspecified. Secondary malignant neoplasm of liver and intrahepatic bile duct. FINDINGS: There is a tiny fat-containing left ventral abdominal wall hernia (image 77 series 2) with an opening measuring approximately 0.9 cm. Tiny fat-containing umbilical hernia (image 75 series 2) is also noted with an opening measuring approximately 0.6 cm. There is a moderate to large ventral colon and small bowel containing hernia with an opening measuring 5.6 cm. No evidence for incarceration or strangulation of bowel is identified. No bowel obstruction is seen. This hernia was also seen previously.  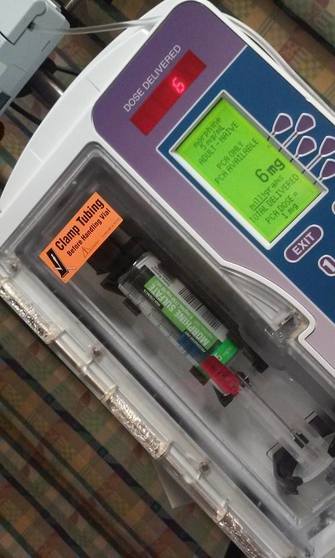   On November 10, 2013, I underwent surgery to remove the left lobe of my liver and to repair my incisional hernia. I was in OR for 9 hours - three hours for the liver and six hours for the hernia. There is no greater joy than waking up and seeing your family at the end of your bed. Originally, the surgery was going to be laparoscopic, but Dr. Jensen, the head surgeon, decided that open surgery was the best way to get at the liver and hernia. Needless to say, I was in a lot of pain and made ample use of my morphine pump. Nan was by my side for nearly the four full days that I was in the hospital. My eagle fan, that I hung from my IV stand, provided me with spiritual protection and nourishment. The operation left me with a 9” incision. Twenty-five staples were used to close it. The best news came from Dr. Jensen. He said I was clean - no other cancer was found on my organs. Once I got home, Nan assumed a strong role as my caregiver. I had a drainage tube attached and Nan had to empty it daily and record how much fluid was collected in the discharge cup. I was also given 28 day supply of Enoxaparin syringes. These were used to prevent deep vein thrombosis prophylaxis to prevent blood clots in the lower leg and thigh. Nan provided me with my daily injections. 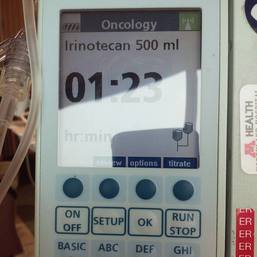 In January 2017, my new cancer regimen included 12 rounds of adjuvant chemo and a high-intensity surveillance program - CT scans every three months for two years followed by two CT scans a year for three years and annual colonoscopies. The Irinotecan chemo was a rugged chemo with side effects that included nausea, vomiting, diarrhea, fatigue, loss of appetite. My hair had been growing back following the cessation of neoadjuvant chemo that was given prior to my surgery. Once I began Irinotecan, my hair turned brittle and began to fall out. I basically suffered total hair loss - loss of head, facial, and body hair. 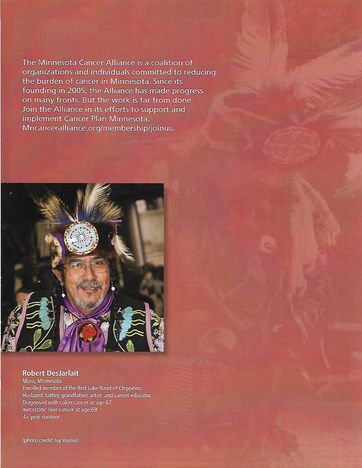 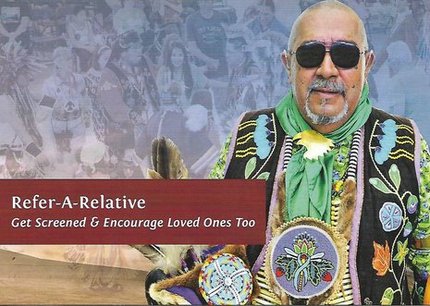  In 2017, I appeared in the booklet "Cancer Plan Minnesota 2025" by the Minnesota Cancer Alliance, and colon cancer promotional material for the American Indian Cancer Foundation. I was featured in publications and articles including "A Community Effort," Cancer Today Magazine (2014); "Meet One Million Strong," Fight Colon Cancer (2014);"Poor Cancer Care for Native Americans Might be a Treaty Violation," Newsweek Magazine (2016). I became a contributing writer at I Had Cancer. My articles include "Cancer is Never Really Out of Sight, Out of Mind" (2017) and "We Are Lanterns In The Darkest Night" (2018). I was also featured on the cover of Mazina'igan (2018), a publication by the Great Lakes Indian Fish & Wildlife Commission.      Powwow for Hope photos / Ivy Vainio In May 2017, my wife/caregiver and I gifted the American Indian Cancer Foundation (AICAF) with an eagle staff at their 6th Annual Powwow for Hope. The eagle staff was created by Nan and I from a dream vision that I had. In turn, I was gifted with a beautiful walking staff. Nan was honored at the Caregiver's Honor Dance and received the blanket "Renewal" by Sarah Agton Howes. 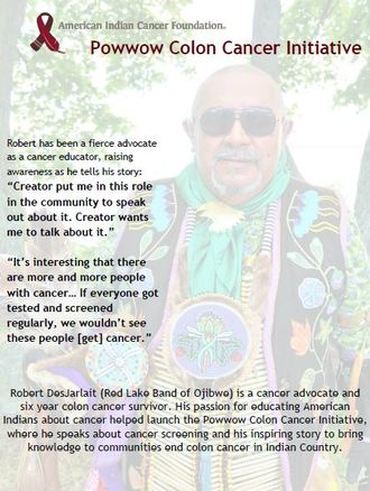  Lake Vermilion Powwow. Photo / Ivy Vainio In April 2018, I became the spokesperson for the Colon Cancer Powwow Initiative. The initiative was sponsored by the American Indian Cancer Foundation through a grant by the Minnesota Health Department. From April to June, we visited six powwows - Osseo Indian Education Powwow, Augsburg Powwow, U of M Indian Students Powwow, Leech Lake Powwow, White Earth Powwow, and Lake Vermilion Powwow. The main focus of the initiative was to tell my survivor story and create awareness about colon cancer, and cancer in general, in Indian Country.  Photo / Stephanie Thompson My main support group is my family - my wife, Nan, daughters, Meeg-wun Giizhig'kwe, Makina Anung'kwe, sons, Miskwa Mukwa and Miziway Migizi, and my grandson, Tae-Tae. But there are many others - extended family members, dear, close friends, and many, many others who I haven't met and may never meet. Without them, my cancer journey would not be possible.  Photo by Ivy Vainio The story doesn't end here. There will be chapters to add in the days and months - and hopefully, years - ahead. New words and photos will unfold. However, being a Stage IV cancer survivor doesn't allow me to look too far into the future. Despite the lingering after-effects and the ensuing cancer PTSD, my lab/blood work show my immune system and organs to be in fairly good shape. The best news is that I've been cancer free for over 18 months. My CT scans since November 2017 have consistently declared NED (No Evidence of Disease): IMPRESSION: 2. Postop changes status post partial hepatic and colon resection are again noted. No new evidence for metastasis or recurrent malignancy is seen. In the meantime I'll continue to tell and live my story until I'm called homeward to the Land of Everlasting Happiness. Until then, I will appreciate each day that is given to me. May the Creator bless you and yours. Mii'gwech.  Photo / Patty Maquire We Are Lanterns In The Darkest Night Whose flames illuminate tales Of paths trodden in the past And of paths to tred yet ahead; Wind nor rain Shall extinguish our light For our stories Will be forever told In the hearts and minds Of those we leave behind.  Photo / Steve Premo Postscript: Chi-mii'gwech to Ivy Vainio for the literally hundreds of photographs that she has taken of me since 2012. The majority of photos in this article, other than mine, were taken by Ivy. Ivy and her husband, Dr. Arne Vainio, are dear friends who have been two of my strongest supporters on my cancer journey. Kiitos to both of you. © All Rights Reserved, 2018, Robert DesJarlait All photos except where noted by the author and may not be used without written permission © 2018, Photos, Ivy Vainio Medical record excerpts and diagrams property of the author. For reproduction information, contact the author at [email protected] 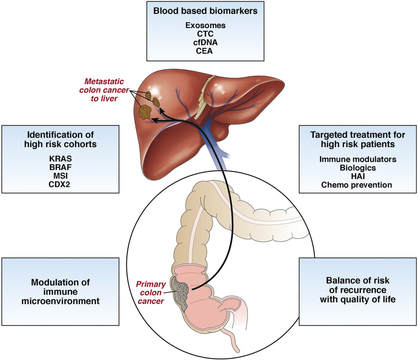 I found out this morning that my cancer is Stage IV. After talking to other survivors and doing my research at reputable cancer sites, I found that my recurrence in 2016 has uncomfortably moved me into the Stage IV category. "If the cancer has spread to distant parts of the body, it is called metastatic recurrence. Metastatic cancer is also called stage 4" (Anne Schott, associate professor of medical oncology at the University of Michigan Rogel Cancer Center). In my case, when my colon cancer spread to the left lobe of my liver, I moved into the Stage IV category. The metastasis didn't occur via my lymph nodes because those were removed when my ascending colon was removed. Rather, the invading cancer cells traveled through my blood stream and established a colony on the left lobe of my liver. It's estimated that should recurrence occur, it usually reappears in the third year following surgery. That is exactly what happened to me. The photo that I included provides a graphic look at colon cancer metastasis to the liver. For the uninformed, there are four stages in cancer:
When I first contracted cancer in 2013, my ascending colon was removed. After the tumor was biopsied, it was classified as Stage I because the cancer hadn’t spread beyond the walls of my colon into the lymph nodes or other parts of my body. As such, chemo wasn’t required. Thereafter, I was placed on a low-intensity surveillance program – CT scans once a year for five years. Why five years? Because the 5-year survival rate for Stage I colon cancer patients is 93%. If you remain NED (No Evidence of Disease) in the five-year timeline, you are then considered free of cancer. For the first two years, I was NED. But in the third year, 2016, my CT scan revealed colon cancer metastasis to the left lobe of my liver. I went through four rounds of neoadjuvant chemo, i.e., chemo before surgery, and twelve rounds of adjuvant chemo following surgery. I was placed on a high-intensity surveillance schedule – CT scans every three months for three years, followed by two CT scans a year for two years. At the present writing, I’ve had seven scans and remain NED. Through all this, I was totally unaware that my status as a cancer patient had changed. I knew I was a high-risk cancer patient, but I didn’t know that in Cancerland parlance, I was a Stage IV survivor. Why didn’t I know? Because I didn’t ask. It’s important to dialogue with your oncologist. I didn’t do my research to have a better understanding of high-intensity surveillance. Had I done so, I could have asked when my oncologist asked me if I had any questions. When it comes to cancer, a patient needs to have an understanding of the type of cancer that they are dealing with, an understanding that enables them to ask questions when talking to their doctor. In my case, I dropped the ball and found out later than sooner. Stage IV almost sounds like a death sentence because “metastatic cancer is rarely curable. Cancer, by its very nature, is designed to spread. Cancer develops when your body's cells go awry and begin reproducing and invading surrounding tissue in a way that nature did not intend. The cancer cells travel to different parts of the body and begin forming new tumors…The goal for treating a spread cancer is to reduce tumor size and relieve some of the symptoms that patients experience. This allows us to prolong an individual's life and, in many cases, allows a person to live a high-quality life” (Anne Schott). And therein is the hope – the hope for a high-quality life despite dealing with metastatic cancer. But with it comes the necessities at looking at my priorities. There are a few things I want to accomplish. So I need to focus on those. Don’t get me wrong. I’m still a long way from journeying to the Land of Everlasting Happiness. But when the specter of death is lurking nearby, there are things you want to get done. As I’ve said before – the cancer journey goes ever on. There are many twists, turns, and tangents on this path. And today, I’ve wandered onto a new tangent. © Robert DesJarlait, 2018
|

Robert Desjarlait
|
 RSS Feed
RSS Feed
