|
On my Manijooshiwaapine Babaamaadiziwin (Cancer Journey), I often view my path from a cultural mindset – an Anishinaabe mindset. To perceive things in this manner helps me to understand the situations that I face. Such a mindset allows me to think in a more positive way that is much needed in this struggle against amogowin (cancer). With this mindset. I refuse to be a victim. Being a victim opens the door to self-pity and all that it entails. I am not about self-pity and, therefore, I am not a victim. I am a warrior who is calm in the face of the storm. Only in calmness can I understand and battle the one I call Awensii (The Beast). There is a story that a good friend told me. His daughter’s life was taken by Awensii. But she wasn’t fearful. Rather, she offered asemaa to her amogowin because it was part of her, a spirit within her. She offered asemaa to her amogowin daily and in doing so, she offered a prayer. Amogowin is, of course, a part of us. It lives within us and feeds on us. It is not an invasive force. It is a dreadful twin that seeks to overcome us, to render death not life. One story that I heard many years ago is called “Our Twin.” It is about the other side that is part of us. It is the evil side of us – a negative force that seeks to destroy us. It is a story given to Nenabozho by Bug-way’-ji-inni (Wildman, also known as Sasquatch) on his journey to the East. I’ve chosen to adapt the story to recognize Amogowin as our evil twin. Amogowin is your other side in all things and in all ways. He is with you…do not seek him. Do not wish to know him but understand him. You will walk the path of healing…he will not; You are kind of spirit…he is not; You are self-love…he is self-pity; You are humble…he is not; You seek healing…he does not; You shall respect others…he will not; You will seek the goodness of heart in others…he will not; You are the Light…he is the Darkness. Like other Manidoog, offer him asemaa to know that he is with you, understand him. But do not seek him.
0 Comments
Of course, the price of cancer could be your life. But this entry isn’t about that; rather, it’s about the cost of cancer in terms of financial responsibilities and obligations to the cancer patient. I can only relate here my own experiences of financial burdens incurred by me on my cancer journey. Everyone has different health providers and, in turn, the state that you live in is affected by the various health care coverage in regard to cancer. However, since a majority of cancer patients are seniors who are on Medicare, then perhaps my experience may help you. I retired from my job in 2007. For two years, I collected unemployment benefits. When those ended, I took early Social Security retirement at age 62. Of course, when you take early SS retirement, your full benefits that you receive at age 66 are diminished by 30%. My early retirement SS benefit was for $806 a month (which is now $906 because of cost of living increases). You can continue to work part-time and earn up $20,000 per year without paying taxes. But I chose to earn a little extra money by doing lectures/presentations and selling some art and writing articles. On the average, my yearly income is around $12,000. So, yes, I live well below the poverty level but I get by with a little hustle. When I turned 65, I qualified for Medicare. You are automatically assigned to Part A – hospital insurance. You have the option of signing for Part B – medical insurance. But you have to pay a monthly premium, and the premium is deducted from your Social Security benefits, or they can paid out-of-pocket. In my case, it was $117. Not a bad deal, but when you’re only collecting $806 a month, it cuts into your meager living expenses. So I rejected Plan B. The catch to Part B is that once you reject it, you can’t sign up for it again. But I had been in good health all my life, largely because of my life as a powwow dancer, and hadn’t suffered any major illnesses. I didn’t expect to have any major health problems in my golden age. So I thought why bother with Part B since I'd never probably need it. So much for self-made, wishful prophecies. In November 2012, I suffered a heart attack at a Thanksgiving powwow at the Minneapolis American Indian Center. I was taken by ambulance to the Hennepin County Medical Center and an emergency angioplasty was performed to install a stent in my left coronary artery which was blocked. One of the thoughts that crossed my mind in my hospital bed was how all this going to paid for? I mean, I had Medicare hospital care, but what would it exactly cover? And there was the question of prescriptions. Under Medicare, if you sign with Part B, you then have the option of signing for Part D – prescription coverage. Since I had rejected Part B, I had also rejected Part D. Two days later, a Hennepin County financial worker came to see me. She signed me up for Medical Assistance. Through MA, the state reopened my Medicare and signed me up for Part B and D, and the state paid the premium for MA. I was signed up for Blue Cross/Blue Advantage for seniors. All the hospital costs for my heart surgery, hospital stay, prescriptions, and clinic visits were paid for. When I was diagnosed with colon cancer in April 2012, I also incurred no costs regarding my surgery, prescriptions, and clinic visits. Also at that time, Blue Cross put me on Blue Plus, a more inclusive program for seniors. Earlier this year, Blue Cross pulled out of the Minnesota MA system. They maintained limited Blue Plus coverage in some counties. I moved to Kanabec County in May 2016. When you move to a different county, you have to reapply for MA. Kanabec County didn’t offer Blue Plus; rather, they offered a HMO SeniorCare Complete or SenCare under their Southern County Health Alliance (SCHA). The medical service type is Medicare. In other words, SenCare functions under Medicare. In July, After I moved to Kanabec County and my recurrence of cancer happened – colon cancer mets to my liver. The total cost so far is $12,972 and includes clinic visits to specialists, CT scan, PET scan, biopsies, and chemo, with no costs incurred by me. My chemo regimen includes an IV infusion of Oxaliplatin and Capecitabine oral tablets. One round of chemo begins with an infusion followed by 14 days of oral tabs. Then I’m off for 7 days before the next round begins. I have four rounds of chemo before my operation in October. So, everything is the same as before, except with one difference. Outpatient chemo therapy isn’t covered. I found out that chemo pills that are part of your chemo regimen and that you take at home are not totally covered. Under Medicare, there is a 20% co-pay for those type of prescriptions. Chemo infusions that are given in the clinic are covered. There is no co-pay for that. I didn’t know any of this when I went in for my third round of chemo (8/19). I was in my chemo chair and the pharmacist came in. He usually brings my chemo prescription pills. But he was empty-handed and asked if I had changed medical providers. When I explained the change in Kanabec County, he said there was now a co-pay. The co-pay was 20% of the cost for the chemo pills, i.e., $350 co-pay for a prescription that cost $3500 for 112 pills. Nan and I were a bit stunned and shocked about the co-pay. Not so much of the co-pay itself, but the cost of the co-pay - $350. The pharmacist took my medical card and said he would make a few calls. Nan and I talked about the situation. We had money in my cancer support fund, so we could use that. However, the cancer support fund was, is, intended for other purposes and unforeseeable circumstances, co-pays weren’t included under unforeseeable circumstances. And we figured we could use the support fund to pay for my fourth and last round of chemo on September 8. The pharmacist came back. He explained that the state pays for Medicare through MA, but under Medicare guidelines, the state only covers 80% for chemo outpatient prescriptions and the patient pays 20%. As it turned out, I had a bit of luck. After my first round of chemo, I had misread the dosage on my pill bottle and was only taking half of the dosage. The dosage is for 4 tablets daily twice a day for 14 days for a total of 112 pills. I had misread it as 4 tablets a day, meaning that I only took half of the prescribed dosage. So, I had 56 pills left over from my first round. The pharmacist only had to fill a prescription of 56 pills to bring it up to full dosage. Instead of paying $350 for co-pay, I would have to pay $175. He also let me bill it since there wasn’t an ATM machine in the building. The nurse said another alternative for my outpatient therapy would be a pump. At home, I would pump the Capecitabine through my port. She said it was cheaper than the pills. The only drawback is it takes 48 for the process and you have to be fairly active during the process. I don’t know exactly what the future holds. I will be on chemo after my operation for four months. I’m guessing that the financial cost, at 20% per round for pills, will be around $1500-$1700. My cancer support fund won’t be able to sustain that. My cancer support fund campaign is still at GoFundMe. It’s presently dormant since I reached my desired campaign goal. But I can re-activate it, and I’ll probably use that option after my operation and try to raise the additional funding that I’ll need. But aside from my own situation, the main point of this column is to raise awareness for seniors on what they can expect if they are on Medicare and should they contract cancer. There will be a 20% co-pay for outpatient cancer drugs, and the higher the cost for the drug translates as a higher co-pay for the patient. There are grants available to help with the costs (I’m not currently eligible for these). Also, many hospital financial workers, and doctors themselves, will help to figure out ways to meet the costs. For further reading, I’ve enclosed a link to the American Cancer Society booklet: “Lifeline: Why Cancer Patients Depend On Medicare For Critical Coverage.”  My IV infusion of Oxaliplatin.  One round of Capecitabine tablets.
Back in the late ‘60s-early’70s, the music of Crosby, Stills, Nash and sometimes, Young, epitomized the essence of the counter-culture movement. Their songs became anthems for us hippies. So many classic tunes that reflected the times – “Wooden Ships,” "Teach Your Children,” “Woodstock” to name a few. And who can forget one of the most defining songs of that era – “For What It’s Worth,” by Steven Stills in his pre-CSNY days with Buffalo Springfield. One song that especially stood out for us longhairs was Crosby’s “Almost Cut My Hair.” His opening lines defined our roles in the counter-culture: “Almost cut my hair It happened just the other day It's gettin kinda long I coulda said it was in my way But I didn't and I wonder why I feel like letting my freak flag fly Yes, I feel like I owe it to someone” Yes, our freak flags defined who were – rebellious, anti-establishment, anti-war, and tuned in, turned on, dropped out on pot and LSD, love and peace. I was 21 when the Summer of Love arrived. I never made it to San Francisco with flowers in my hair. But we had our own hippie scene on the West Bank at Minneapolis. I grew my freak flag and let it fly, strolling the streets in bell bottoms and love beads, with my head abuzz with that sweet , enchanting mistress Mary Jane. For me, my freak flag came with a bonus. I was Native American and it connected me to my identity as an Anishinaabe man. And as the counter-culture faded and freak flags lost their meaning, my hair switched meaning – it formed the basis of who I was, where I came from, and where I was going to. As an urban Indian, I knew very little about the traditional heritage of my people. The village where I was born, Ogaakaaning (Place of Walleyes / Red Lake) Miskwagamiiwi-zaaga’iganing Ishkonigan (Red Lake Reservation), had been heavily Christianized as a result of colonization and assimilative policies. Niinizisimaa (My hair) became a transition point that marked the beginning of my search to connect with my Anishinaabe Spirit. And it became part of my identity for the next 48 years. Niinizisimaa, untouched, would have gone with me to Gaagigi-minawaanigoziwining (Land of Everlasting Happiness) until The Beast entered my life a second time with a recurrence of amogowin (cancer). Recurrence meant chemotherapy and chemotherapy meant side effects. I knew that chemo meant that I faced the potential binaandibeshkaa niinizisimaa (loss or partial loss of my hair). As a dancer – and I’ve danced for over 32 years – I wore niiinizisimaa (my hair) in abikaanan (braids) and a wiinikway (scalplock). When I wasn’t dancing, nibikwapijige (I wore my hair in a ponytail) along with niiinikway (my scalplock) which I often left in my hair after dancing. In dance, I represented an ogichidaa (warrior). The wiinikway was an essential link to the ogichidaag spirit and traditions. Long ago, ogichidaag (warriors) would use bear grease or birch bark to make their wiinikwayan stand up. When they engaged in battle, they would lower their heads and wave their wiinikwayan toward their opponent to taunt them. And when it came to scalping, it was the wiinikway that was taken rather than the entire scalp. On the morning of my port insertion, I had made my decision to nigiishkikozhiwe (cut my hair). I decided that rather than letting The Beast take niiinizisimaa (my hair) , I would do it myself. As we waited in the lobby, I asked wiijiiwaagan (my wife) Nan to braid my wiinikway. Then I handed her a scissors and told her to cut it. At first, she didn’t want to, but I said it was okay and this is the way it has to be. I put niinikway in a plastic bag and asked her to keep it in her purse. As we waited, I turned to her and said: “Man, you got my scalplock…you can put all kinds of medicine on me.” Then I said: “Dang, you got complete control over me.” She looked at me and said: “I had control of you since the day we met.” Initially, the plan was to get my hair cut after I was done with port insertion and infusion. But it grew into a long day and didn’t have time to go to the barber. The next day, I got up, brushed and gathered my hair into a ponytail, and cut it off. It was hard, very hard. I looked at my ponytail on my bed. And I cried. My ponytail had been with me for many years. I thought about The Beast and how The Beast had brought me to this point. But there was no shame in my tears. Because tears are part of healing. I began thinking about how our ogichidaag (warriors) jiigindibebizhiwe (took the scalps of the enemy) and brought them back to the village. They would have a feast to honor the jiigindibebizhiwe and thereby honor the jiibayag (spirits) of those lives that were taken. This would be followed by a jiigindibebizhiwe-niimi (scalp dance) with the jiigindibebizhiwe attached to a dakobijigan (hoop). Thereafter, the jiigindibebizhiwe dakobijigan would be taken care of by the family of the ogichidaa who had taken jiigindibebizhiwe. After removing my own scalplock and ponytail, it became clear to me the meaning of all this. Niiinizisimaa (My hair) represented my own achaak (spirit) and it now became my responsibility to take care of it and after, taken care of by my family. It represented my war path against The Beast. But in my case, The Beast didn't take it, I did. The Victory Dance belonged to me, not The Beast. Out of my tears, I found a measure of truth. An hour later, I walked down the street to the local barber to complete my task. He was an old guy and was surprised when I told him I wanted my head shaved. He said: “For a 70 year-old man, you have some beautiful hair. You sure you want to do this?” I said I was a cancer patient, taking chemo, and I wanted to put off the inevitable. When he was finished, he did as I requested, and put my hair in a plastic bag. I'll take this hair from the barber and release it on Mississippi. I remember Ona Kingbird, an elder from Red Lake, saying to make your offerings on that river because of our connection to it. She also said there is a special connection to that river regarding Anishinaabe'kwewag. And when you make an offering to remember the women in your family...especially indoodoo (my mother) and nookomis (grandmother). So the journey continues. And I reach out to our traditional teachings to help me with the healing. Because that is the way I’ve been taught.  Niiinizisimaa - My scalplock representing my status as a warrior in dance.  My ponytail with my scalplock. Cutting off my ponytail was the most difficult thing that I've had to do on my cancer journey. But doing so provided me with a teaching, a waking vision, that brought balance on my path.  The hair that was cut at the barber shop. This too came with a teaching, one that I will honor.  Self-Portrait as a Cancer Warrior
Amogowin (Cancer) changes your body. I’m not just referring to the organs that are affected by amogowin or portion of organs that are removed surgically or shrunk by mashkiki gaa-aabadak ji-nichigaa deg manijooshiwaapinewin (chemotherapy) and/or angwaakizigaade gaa-zanagak aakoziwin (radiation). I’m speaking about the physical changes – visible scars that form and shape our new lives as cancer survivors. For me, the most visible scar is related to the giishkizhogoowin (incision) made for my gaa-zanagak aakoziwin odayaan imaa gaa-onji-miiziid maajizhwaaganiwi (colon cancer surgery) in May 2013. It isn’t the scar itself, but rather what developed in relation to the maajizhwaaganiwi (surgery) and the giishkizhogoowin (incision) that was made for access to gaa-onji-miiziiyin (my colon). A vertical giishkizhogoowin (incision), approximately 3”-4”, was made from the top of indis (my navel). The type of maajizhwaaganiwi (surgery) performed was a laparoscopic colon resection. The 10 mm gaa-bikoging gegoon (tumor) was located in my cecum. The cecum is located at the bottom of the ascending colon. Approximately one-foot was resected or removed. Or more specifically, my ascending colon was removed. I was left with three scars – the giishkizhogoowin (incision) above indis (my navel) for the laparoscopic scope/camera, and two dime-sized scars for the laparoscopic tools – one near nidisinaake (my sternum) and one on the left side of nimisad (my abdomen). After several months, I noticed a lump on the right side of the cancer scar at indis (my navel). Of course my first thought was The Beast had returned. But that didn’t seem likely since my cancer was diagnosed as Stage I colon cancer. A year passed and I went to my first annual zhaabwaateshimaaganiwi mamaand waabik e-aabajichigaadeg dago (CT scan) and biindaabiiginigaadeni mazinaaki ziganens o-gichi-onagizhiing jiwaabanjigaadenig ji-aakozigwen (colonoscopy). By then, the lump has increased in size. I called the lump my baby bump. My mashkikiiwinini gaa-zanagak aako-ziwin gaa-dazhiikang (oncologist) and the ikwe-mashkikiiwinini (doctor) who did my surgery said that the lump was an ozhigwii (hernia). Apparently, it’s a common condition for those who have had laparoscopic colon surgery (and a common condition for others who have had laparoscopies in the abdomen area.) I was told to take it easy and not lift anything heavy. The only concern was if it became inflected. In that case, I was to seek immediate medical attention. Of course, I didn’t limit my activity. We moved twice and although I avoided lifted the heavier items, I did do some lifting. And then there were household chores that sometimes required some lifting. As a result, my ozhigwii (hernia) increased in size to a large, soft knot. But there was more. My entire abdomen area took on an odd, asymmetrical shape. My recent CT scan (5/23) narrative noted these changes: “Interval enlargement of ventral hernia containing omental fat and nonobstructed bowel loops, the neck remains widened measuring up to 7 cm.” My PET scan on 5/24 noted: “Postoperative changes of proximal colectomy with an unchanged left paramedian ventral hernia containing multiple loops of small bowel. There is no evidence of strangulation or bowel obstruction.” Said another way, the visible, protruding knot on my abdomen is just the tip of the hernia iceberg; the asymmetrical shape of my abdomen is also part of the hernia. Given the situation, my oncologist added Michele Montejo Loor, MD, to my cancer team. I met with her on 7/18 to discuss the procedure for maajizhwaaganiwi ozaam e-gii-zhigwiid (incisional hernia repair). She explained that when surgery is performed in the abdomen area, a gap or opening is created in the abdomen wall. Fat and muscle pushes through the gap and creates the hernia. Dr. Loors will use the laparoscopic method, although she may use both the laparoscopy and conventional methods – it depends on what the laparoscopic camera reveals. She expects the surgery to take four hours. Her surgery will be immediately followed by liver surgery, and that is expected to take two hours. On October 10, I’ll be meeting with Dr. Greeno, the oncologist who is the head of my cancer team, and with Dr. Jensen, who will lead the surgery teams and who will do the surgery to remove the lesion on my liver. I expect surgery will be scheduled for mid-October. Did I say Fuck Cancer? 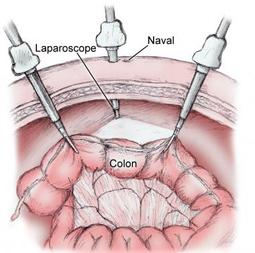 Laparoscopic Surgery. 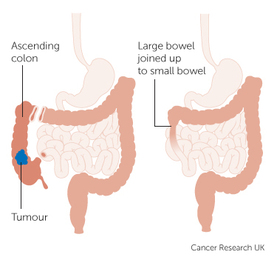 Ascending colon resection. 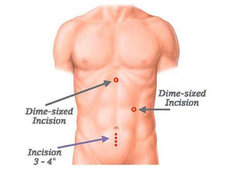 Incision marks for laparoscopic surgery. In my case, the incision for the scope was above my navel.  Collateral Damage.  It may look painful, but it's not. There are no nerve endings because those were cut for surgery. The knot is the most visible part of the hernia; however, the asymmetrical shape under is also the hernia. That will be removed. A mesh will be placed over the knot and the loose flesh will be folded together and stapled. A little nip and tuck, although this isn't for being obese.
On 7/28, I returned to U of M/Fairview and Masonic Cancer Clinic for a long day of interrelated appointments that revolved around my second round of chemotherapy. My first appointment was at U of M for port insertion. Of course, I know that people that are dealing with cancer know what a port is. But there are others who may face cancer at some point, and port insertion may be one of the roads they will cross. Ports aren’t limited to cancer treatment but for other IV therapy treatments. This includes power injected contrast for CT scans and to withdraw blood for blood lab. In regard to cancer, chemotherapy drugs are administered by IV infusion and/or orally. My chemo regimen includes both - Oxaliplatin, IV infusion and Capecitabine, oral tablets. Each round of chemo includes an IV infusion followed by 14 days of oral tabs (8 per day). After 14 days, there are 7 days off before the next round of chemo begins. Currently there are three rounds of chemo with my last one on August 18. There will be a six week break, surgery in early October, followed by four months of chemo. I wasn’t aware of ports until I read about them at Blue Hope Nation, a Facebook page for colon cancer survivors. When my RN cancer nurse brought up the topic at my first infusion, I decided to have the port insertion. Although I was long accustomed to jabbing, it made sense to have port insertion and have one less problem to deal with. Port insertion was scheduled for my next visit, before infusion. At 6:30 a.m., I arrived at Interventional Radiology at U of M/Fairview. My nurse drew blood for blood lab. The doctor who would perform the procedure visited me and explained the procedure. I signed the release forms and I was then prepped for the port insertion surgery. The nurse showed me the port. The port was a triangular shape with a white tube attached. Two incisions would be made. One incision was for the port…a small “pocket” is made to hold the port and then sewn up, i.e., the port is completely under the skin. The other incision was for the catheter, i.e., the tube, which would be inserted in a neck vein. They wheeled me into the surgery room at about 8. I was given a local anesthesia. Although I was slightly sedated, I was awake and aware throughout the entire procedure. It took about an hour, and then I was wheeled back to my exam room. During the procedure, I was given an IV cocktail of steroids and an anti-nausea agent. When the nurse came to see me, she asked if I needed anything. I said, sure, a T-bone steak and mocha. She laughed and said, we don’t offer that, but I can get you some toast and juice. I said that was fine (I was famished; I had to fast 6 hours before the procedure). I was kept in observation for an hour. I was given instructions about bathing – no baths and only showers with my back turned to the shower head. (I didn't ask the obvious question - how can you get clean if your back is turned to the shower.) Said another way, it meant no bathing for several days. They wanted me to keep my incisions clean and dry. When I was released, I got on the shuttle and headed over to the Masonic Cancer Clinic for my chemo infusion with my new Port of Dez in the Tropic of Cancer.  The packet I received with my port insertion. It also includes a card that I carry with me should I need to show other medical providers that I have a port and the kind of port I have. The Smart Port is the newest port technology available.  The port and catheter. When I first saw this, I said, Hey! The Vikings! But the nurse said, no, yours will be white. So much for reppin the Vikings in my chest. Via two incisions, the port and catheter are placed completely under the skin. Once I've completed chemotherapy, I can have it removed, or I can keep it. I'm leaning towards keeping it - just in case.  My first infusion at the Port of Dez on the Tropic of Cancer  I call these scars my Purple Heart - wounds that Ogichidaag Amogowin (Cancer Warriors) receive in battle with The Beast.
|

Robert Desjarlait
|
 RSS Feed
RSS Feed
