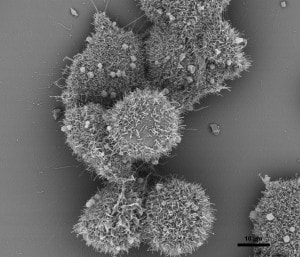
 The nature of The Beast - Colon cancer cells. Cancer survivors have an understanding of each other. We belong to an exclusive club. It’s not a club that you strive to join. “You have cancer” are the three words that gain admittance to the club - and surviving, of course. We don’t do high-fives when we hook up with each other at our local cancer clinic for appointments. Those are usually somber affairs. But social media has allowed us to communicate with each other. We join online support groups that allow us to talk to one another about our experiences, about chemo, and about our oncs. We have our own language - onc(s), scanxiety, NED among other words. Many of us have our own name for our cancer. I call mine The Beast. We don’t distinguish between races because cancer is a disease that knows no racial or class boundaries. One of the things we celebrate is when our CT scan is NED. NED means No Evidence of Disease. More specifically it means that our cancer is in complete remission. It doesn’t mean we’re “cured” of cancer. It means that cancer hasn’t been detected by the scan. Yet, there are nagging doubts about NED and complete remission. Go to any cancer support group and you’ll hear those doubts expressed. It is probably one of the most talked about topics among survivors. It’s not that we don’t have faith in our doctors. We’ve lived in the bright sunshine of survivorship until a dark cloud of recurrence blots it all out. And recurrence happens to too many of us. As a Stage IV survivor, I’m inquisitive about this disease that I have. I spend a lot of time reading books and articles about The Beast. I do so because I want to know my enemy. Recently I read “The Death of Cancer” by Vincent T. DeVita Jr., M.D., and Elizabeth DeVita-Raeburn. It’s not the type of book that most survivors would read. Unless, like me, they are inquisitive. It’s not bogged down with indecipherable scientific/medical terms. It’s a well written memoir, understandable, and a page-turner. One early passage made me sit up: “But we have to be smart about what we hit them with – and how aggressively. Cancer cells are uncannily adaptive; they learn to outwit therapies quickly. So the first attempt to treat a cancer has the best odds of curing it, because we’re hitting it with something it’s never seen before. The cancer is more treatable than it will ever be again. This is one reason why recurrences are so troubling: you’re dealing with much smarter cells by then.” The last sentence was particularly troubling to me because of my own recurrence in 2016. My recurrence was a surprise to me and my onc. But I’m jumping ahead in my narrative. I have to go back to the beginning to where this all started before I can get to the two and a half billionth cell. My sojourn in Cancerland began April 16, 2013. As a result of anemia and black, tarry stools, my doctor at the Native American Community clinic, Katie Bickel (ANP), referred me to Dr. Melton-Meaux, a colon and rectal specialist at U of M Physicians. A colonoscopy was performed on April 26. The pathology results of the colonoscopy were “Malignant partially obstructing tumor cecum.” Alarmed by the results of the colonoscopy, Dr. Melton-Meaux ordered a CT scan which was performed on May 1. The results of the scan were a “lobulated mass involving the distal cecum and ascending colon consistent with known colon carcinoma…There are multiple lymph nodes in the medial mesentery to ascending colon. The size and number are worrisome for possible metastic involvement.” Because of the size of the tumor and its location, Dr. Melton-Meaux decided that surgery should be done as quickly as possible. On May 14, she performed laparoscopic surgery and removed my ascending colon and associated lymph nodes. The surgical pathology report from May 16 states that the tumor was Adenocarcinoma, i.e., the type of tumor in my colon. Adeno means glands and carcinoma is the type of cancer. Adenocarcinoma develops in the lining of the colon (or rectum). The size of my tumor was 9.5 x 5.5 x 3.0 cm and the gross measurement 2.5 cm. It was considered to be a very large tumor, hence Dr. Melton-Meaux's urgency in performing surgery. There was a bowel wall invasion with the tumor infiltrating into it, but not through the muscularis propria. The muscularis propria is a deep, thick layer of muscle that contracts to force along the contents of the intestines. The lymph nodes were all negative, meaning the cancer hadn’t invaded them. Under AJCC Cancer Staging, my cancer was listed as T2, N0, M0, G2. More specifically, T2 means that cancer has grown into the muscularis propria; N0 means no cancer in nearby lymph nodes; M0 means that cancer has not spread to other parts of the body, i.e., no metastasis; and G2 means the cells are somewhat like healthy cells and are called moderately differentiated. Cancer is divided into four stages - I, II, II, IV. Mine was classified as Stage I: The cancer had grown through the mucosa and had invaded the muscular layer of the colon. It had not spread into nearby tissue or lymph nodes Following my surgery I was assigned to an oncologist, Dr. Edward Greeno, to handle my case. In his first oncologist report, Dr. Greeno wrote: Stage 1 colon cancer. The patient has had a complete resection. His risk of recurrence is quite low. His risk is low enough that he need not worry about adjuvant chemotherapy. We should have some minimal followup to watch for evidence of recurrence. I recommended a CEA level and physical exam every 3 months until we are 2 years out, and then every 6 months until we are 5 years out. According the American Cancer Society, the 5-year relative survival rate for people with stage I colon cancer is about 92%. What this means is that an estimated 92 out of 100 people who have colon cancer are still alive 5 years after being diagnosed. However, many of these people live much longer than 5 years after diagnosis. Things were looking pretty good. I was in a group with a high survival rate and chemo wasn’t required. My surgeon, Dr. Melton-Meaux, tacked on yearly colonoscopies as part of my 5-year surveillance program. This was because in a post-surgery colonoscopy on May 28, 2014, multiple hyperplastic (non-pre-cancerous) polyps were removed. Overall, my cancer team was taking good care of me. I didn’t take my annual colonoscopy on schedule in 2015. I waited until January 2016. Three polyps were removed - two were hyperplastic and one was an adenoma polyp. Adenoma polyps are pre-cancerous. They can take seven to ten years to develop into cancer. An adenoma polyp was how it all started for me. Prior to my surgery in 2013, an adenoma polyp had evolved into a tumor. It had been incubating in my colon for seven to ten years. Had I gotten a colonoscopy in my fifties as recommended, I wouldn’t be writing any of this. Almost three years later, cancer was once again trying to reestablish itself in my colon in the same manner that it did previously. It wasn’t cancer per se. It wasn’t recurrence. But the conditions were ripe for it to become cancer in several years. Of course, this was worrisome to me. I thought I was done with The Beast. But here it was again trying to make a reappearance. In May 23, 2016, I had my annual CT scan. It was the third scan of my 5-year surveillance program. I expected it to be like my previous scans - uneventful and NED. I had the scan early in the morning and met with Dr. Greeno in the early afternoon for the results. After greeting me, the first thing Dr. Greeno said was: “Well, Robert, we found something on your scan.” Both my wife and I were crestfallen. We knew this wasn't going to be good news. What was found was a secondary malignant neoplasm of the liver. My colon cancer had metastasized as a lesion on the left lobe of my liver. Dr. Greeno ordered a PET scan for the next day to see if the cancer had metastasized elsewhere, e.g., the lymph nodes. It hadn’t. As a result of my recurrence, my status as a cancer survivor changed to Stage IVA, meaning the cancer has spread to another organ. The 5-year survival rate for Stage IV is 13%. Although the outlook is poor, the cancer can be held in check, i.e., remission, with treatment if the cancer is limited to a small area. In my case, the recurrence was limited to the left lobe of my liver. When I asked Dr. Greeno how the cancer had reached my liver, he said the cells had to have passed through my bloodstream. The occurrence of such is extremely low with Stage I, but it does happen. With my recurrence, the two and a half billionth cell had found its mark. In his book, Dr. DeVita writes: It is unrealistic to use survival as an end point. Consider the number of cancer cells a drug has to kill to be effective. The average patient with advanced cancer has more than a kilogram of tumor on board. That’s many billions of cancer cells, because a lump about one centimeter across contains roughly one billion cells. Even after surgery, when a primary cancer has been removed and no errant cells can be detected, a patient can have more than a billion cancer cells circulating around the body. Consider that the original gross measurement of my colon tumor was 2.5 cm. This would mean that there were roughly two and a half billion cancer cells in my tumor. Granted, the tumor was removed and, along with it, billions of cancer cells. However, as DeVita notes, more than a billion cells continue to circulate in the body. My use of the term “two and a half billionth cell” is simply a point of reference. The main point is that errant cancer cells circulated in my bloodstream and made their way to the left lobe of my liver and established a beachhead. The treatment for my recurrence included four rounds of neoadjuvant chemo - Oxaliplatin infusion with daily doses of Capecitabine tabs. Originally, six rounds of infusion were scheduled; however after a severe reaction to round four, the neoadjuvant chemo was cancelled. In November, 2016, the left lobe of my liver was removed via open surgery. I was in OR for nine hours. Three hours for the liver surgery and six hours to remove an incisional hernia that had developed after my colon surgery in 2013. My liver surgeon, Dr. Eric Jensen, said I was clean - no other cancer was found in my body. I then went through twelve rounds of adjuvant chemo - Irinotecan, which is used for metastatic colon cancer. I was put on a high-surveillance program – CT scans every three months for two years followed with CT scans every six months for three years. My scan this month (October) will complete the two years of my surveillance program and then I will go to the three year program. Of course, I’m comforted by my doctors keeping a watchful eye on me. Yet, there is the nagging thought that I am just another two and a half billionth cell away from metastases. But in writing this, it isn’t my intention to be a cancer doomsayer. There is always uncertainly living with cancer. Yet, today there are targeted treatments and immunotherapy that can provide a survivor with a good, quality life. There may never be an overall cure for cancer, but today’s advancements allow us to manage it and live with it. Complete remission may be the talk of the town in cancer support groups. But that's because we know the reality of complete remission. The two and a half billionth cell is still there. In some cases, it will find us, in other cases it will be held in check with treatment. For survivors, we know that somewhere deep The Beast lurks. Approach it with a respectful fear. But live life as the Creator intended. © 2018, Robert DesJarlait
0 Comments
 I met Herb Sam in 1982. It was the first year of my sobriety and my path on the Red Road. I saw Herb at several feasts in the Native community where he offered the invocation for the food. He spoke in the language and, for me, it was the first time I heard it spoken. At that time, I went to A.A. in North Minneapolis. One of the reasons I chose this particular club, the Mustangs Club, was because I wanted to be around other Natives who were finding their sobriety paths. Many of us were urban Natives and knew very little about our traditions. At that time, there was emphasis on connecting traditions with sobriety. At our table, we often brought up traditional beliefs, trying to connect them with whatever Step was the subject for the evening. But that created friction with non-Native members who felt that Natives were taking over the club. After several months, we decided to establish our own club and moved to the Upper Midwest American Indian Center. We invited Herb to our first feast. He provided a prayer and then talked about sobriety. He told us that we were on the right path and that we had many things to learn and many traditional values to instill in our lives. He said to be patient, that it would take time, and to seek out elders for advice. He then lit his Opwaagan (Pipe) and offered each of us to draw smoke from it. It was the first time I smoked an Opwaagan and it was a powerful experience. It seemed as if the manidoog (spirits) had entered me and soothed my soul-spirit. A few years later, when I started dancing, I saw Herb at the powwows with his Mississippi Ojibwe drum. Him and Chops always at the drum, singing those sweet, old traditional songs. After Chops passed on, it was never the same drum and Herb eventually stopped bringing it to powwows. I think it was about in 2004 that I approached Herb at a powwow, gave him tobacco, and asked if he would give me my name. I was hesitant at first. You always hear stories about how some elders will turn down a request. I was 58 years old, and with the exception of a childhood Ojibwe name from my Godfather, had never received my proper Ojibwe spirit name. Receiving a name is a significant part of an Ojibwe person’s life. With a name, you become a whole person. So I was nervous and hoping that Herb wouldn’t refuse my request. It was with great relief when Herb accepted my tobacco. He said he would have to have a dream first and my name would be revealed in the dream. Once he had the dream, he said he would call me and we would arrange for a naming ceremony. About a month later, Herb called and said he had my name. I wanted to say, what is it? But that would have been foolish. A name has to be properly brought into the world. A few weeks later, Herb came to our house. As per Herb’s instructions, I had a blanket on the floor with food for our feast - traditional foods like blueberries, manoomin (wild rice), frybread (which isn’t traditional, but what’s a feast without frybread?), roast beef (venison wasn’t available) with mashed potatoes and gravy. Herb brought his hand drum. I sat across from him on the blanket and my family sat around us. He told me my name and then explained what the name meant. “Endaso-Giizhik - Every Day. This is the name I dreamed about. It’s a good name. Four warriors had this name. Two were from a long time ago, long before we came here. Every day they went out early in the morning, looking for signs of the enemy, protecting their village. The last one to have this name was an old man who was always at powwows with his children. He reminded me of you - always at powwows with your children. The spirits will know you by this name. Every day remember your name. Every Day do something for your people to help them and protect them.” Then he stood up and with his hand drum sang in each direction, beginning with the east, and sang my name into existence. We then feasted and I gave him tobacco and a blanket for the naming ceremony. Afterward, I put out a spirit plate. In the following years, he gave me advice on personal situations. These weren’t things you could talk about on the phone. Herb’s rules were you had to go see him, bring him tobacco, and only then would he talk to you about the problems you were having. But that’s the way things are done by elders. One of Herb’s attributes as an elder and spiritual man was his work with the Twin City Native American community. He was always at various Native functions offering invocations, and willing to help and provide guidance for organizations and individuals. He lived with his wife, Patty, in Minneapolis, but even after moving back to his home rez, Mille Lacs, he continued his work in the urban community. Herb provided us with a link to our traditions. One of the things he did was to conduct Spring Ceremonies at the Minneapolis American Indian Center. Spring is a time of renewal. It was a time to bless the sacred items you had - Opwaaganag (Pipes), Medicine dresses (Jingle dresses), feathers, dance regalia, and drums - and to feast them. Everything was set out in a circle. Herb stood at the center. He spoke first in English to explain why we were there and what he was doing. Then he spoke in the language, lit his pipe, walked to each item/bundle, and said a blessing prayer for the item(s). Following the ceremony, we had a feast. Herb always asked that we try to bring something traditional. I always brought manoomin. One year, I bought manoomin with waawaashkeshiwi-wiiyaas (deer meat) and miinan (blueberries) mixed in; another year, I brought manoomin with ogaa (walleye) and miinan mixed in. I remember how good the kitchen smelled the night before the ceremony with the aroma of manoomin and deer meat or walleye frying. I wanted to eat some of it but Herb said you shouldn’t eat the food you were going to offer at the feast. It was part of a sacrifice that you were making. At one of the Spring Ceremonies, Herb and I sat off to the side before the ceremony began. If people wonder what old men talk about, it’s almost always about their health. Herb talked about his diabetes. He said he had medicine for it but key element was diet. He said that if people had healthy diets and didn’t eat all the junk food that was out there that diabetes would be less of a problem for our people. Then we talked about my cancer. The previous year, I had cancer surgery. Herb was concerned about it. He said I needed to take care of myself for my family. Then he said something that surprised me. He said cancer was a spirit and that I needed to respect it. He said that cancer was a fearful disease, but by respecting it, I could lessen my fear. Those are words that I took to heart and they became a part of my survivorship and cancer journey. A few years later, Herb became the spiritual advisor for the American Indian Cancer Foundation’s (AICAF) annual Powwow for Hope. In 2017, he blessed the eagle staff that my wife and I gifted to AICAF. On September 14, 2018, Herb passed to the spirit world. In Ojibwe culture, we don’t call it “the Happy Hunting Ground.” We call it Gaagige-minanigoziwining - the Land of Everlasting Happiness. His manner of passing was ironically from cancer. As such, I never expected to be writing about this. I had always thought that Herb would be conducting my funeral. But now that will never happen. We have lost a great warrior and a champion of our people. A generous man who epitomized kindness, humbleness, love, and self-love. We often talk about the Anishinaabe Spirit. The Anishinaabe Spirit is about our personal self, our soul-spirit, and how we conduct ourselves in our daily life. For those of us who know him, we are his legacy. And it is up to us to live within that spirit that Herb taught us about. Mii sa go © Robert DesJarlait, 2018
 Cancer Feathers at Bad River Manoomin Powwow / Photo - Bemused Photography and Design My name is Robert DesJarlait. My Ojibwe name is Endaso-Giizhik. Gichi-miigwech to the Bad River powwow committee for the opportunity to speak for the American Indian Cancer Foundation eagle staff. Although I'm not a veteran, it’s always an honor to be among the veterans bringing in their staffs and flags at the beginning of a powwow and to dance next to those who have served to protect our tribal nations. Eagle staffs represent veteran organizations. Other staffs represent families and community organizations. Together, these eagle staffs represent the indigenous people of Turtle Island. I’ve been an eagle staff bearer for many years. I am the Keeper of the Cherish the Children eagle staff. This summer I’ve traveled to powwows with the American Indian Cancer Foundation eagle staff. I’ve been to powwows throughout Minnesota with this staff. Bringing it to Bad River is significant because it is the first powwow I’ve brought it to outside Minnesota and it will be the last outdoor powwow that I’ll be bringing it to for the year. The cancer staff was made by my wife and me. It was based on a dream vision I had. We made the staff last year and gifted it to the American Indian Cancer Foundation at their Powwow for Hope. There are 15 bald eagle feathers on the staff. Each feather represents one of the 15 major cancers such as breast cancer, lung cancer, childhood cancer, and colon cancer among others. Each feather is wrapped in the color for that cancer. Although 15 cancers are represented, there are 100 types of cancer with over 100 subtypes of cancer. The panel that the feathers are attached to is purple. Purple is the color for all cancers. The golden eagle feather on the tip is for the caregivers. Caregivers are the ones who help take care of us, who get us to our appointments, remind us of our medications, and encourage us to eat healthy foods. The work they do can be difficult and hard. My wife is my caregiver. Without her, I wouldn’t be here. I’m a Stage IV cancer survivor. In 2013, part of my colon was removed. In 2016, a tumor on my liver was removed and I went through 16 rounds of chemotherapy. Last year, when I came to the Bad River powwow, I was bald, had no body or facial hair, and was going through chemo side effects. I was sick from the chemo but I had a commitment to be here. We have high rates of cancer in our communities. Every day it seems like someone gets cancer or passes on from cancer. I personally know several people who have contracted cancer in the past few months. It's a disease that deeply affects our people. Many people don’t talk about cancer. For others, the word is a stigma. It’s as if you mention the word and you will get cancer. It’s important that people become more educated about cancer and talk about it. Learning about the symptoms and signs of cancer can help to prevent it. And save lives. Miigwech for letting me speak for the cancer feathers. Mino ayaa sana Anishinaabedoog.  Posting the AICAF eagle staff at Bad River / Photo - Bob Jauch  Speaking for the cancer feathers at Bad River / Photo - Ivy Vainio Note: Several people requested a transcript of my speech. The short speech that I gave at Bad River wasn't written out. As such, this is the best as I remember it. Whenever I'm asked to speak, I do so in the manner of Ojibwe orators. The words aren't written but rather spoken from the heart. © Robert DesJarlait, 2018
Photos / Courtesy of the photographers How powerful is hope? For me, the power of hope was expressed in a recent status that I posted on Facebook: CT scan results - NED. Stage IV Survivor - 18 months cancer free. I posted my status on my Timeline and at Blue Hope Nation, a colon cancer support group. My status generated over 730+ responses. I had expected a few hundred responses, but never the number that flowed in throughout the day. I clearly underestimated the power of hope to others. That’s not to say that I misunderstood what hope means to cancer survivors. Many of us know that hope is a life lived in remission. Hope for another day, another week, another month, another year. For some, remission can last for years. But hope doesn’t come easy. In May 2013, my ascending colon removed through laparoscopic surgery. I was fortunate because the tumor didn’t breach the walls of my ascending colon and invade my lymph nodes. I was Stage I with no need for chemo albeit I was considered a high-risk cancer patient. Low-intensity surveillance followed - one CT scan a year for five years. Once I reached that five-year benchmark, I could consider myself as cancer free. I had great odds - 93% five-year survival rate for Stage I survivors. Then, in my third year CT scan, to the surprise of my oncologist, the cancer reappeared in the left lobe of my liver. My initial hope of being NED for five years was dashed. My designation as a survivor changed to Stage IV. And my battle with The Beast was renewed. The new battle began with four rounds of neoadjuvant chemo - monthly infusions of Oxaliplatin with a daily intake of Capecitabine tablets. In November 2016, I was in OR for open surgery for nine hours - three hours to remove the left lobe of my liver and six hours to remove a large, incisional hernia that was a result of my 2013 colon cancer surgery. My adjuvant chemo consisted of twelve rounds of Irinotecan followed by a high-intensity surveillance program of CT scans every three months for two years and two CT scans a year for three years. So now I am back to the five-year program. Certainly I’m battle-weary. The surgery has scarred my body and the chemo has left its mark. But scars, cancer PTSD, lingering after-effects, and peripheral neuropathic problems are a small price to pay for my renewed hope. On my journey, I’ve learned that you have to face death to know the value of life. Cancer survivors know all about this. We live a life of hope because our hope is predicated on death. And death has dwelled within us. Our experience with death isn’t objective. Our experiences are subjective. Death has spoken to us through our mutated cells, diseased organ(s), and the scars on our body. Conventional medicine can remove the tumors and diseased cells, but it is hope that guides our spirits. I’ve found that my hope has become the hope of others who have to deal with this daunting and insidious disease. This was best summed up by a survivor who responded to my post: “Wonderful! Thanks for sharing and giving newbies HOPE! Celebrate.” Yes, I will celebrate. Each and every day, I will celebrate. That is the power of hope. Sometimes on the field of battle, victory isn’t measured by the relinquishment of the foe. Rather, it can be measured by the depth of one’s hope. And that is a depth that reaches far into one’s heart. © Robert DesJarlait, 2018
Once again, FB (Facebook) armchair oncologists are busy posting an article that purports to warn people about the dangers of chemotherapy. The headline is an eye catcher – “Shocking New Study Shows Half of Cancer Patients are Killed by Chemotherapy, Not Cancer.” Never mind the fact that the study came out in 2016. Alt-med sites, with their unending war against chemo, have regurgitated the study and time-stamped it as August 2018 to give it the veneer of current information. In turn, FB armchair oncologists re-post the “current” article and enable the alt-med circle of misinformation to continue unchecked. By unchecked, I mean that alt-med proponents and armchair oncologists don’t bother to read the actual study. To do so would undermine their idea that chemo kills people rather than save lives. And alt-med doesn’t want to sell the idea that chemo can save people. Rather, they would have you believe that their alternative medicine remedies will save you. The study in question is “30-day Mortality after Systemic Anticancer Treatment for Breast and Lung Cancer in England: a Population-based,Observational Study,” Michael Wallington, Emma B Saxon, Martine Bomb, Rebecca Smittenaar, Matthew Wickenden, Sean McPhail, Jem Rashbass, David Chao, John Dewar, Denis Talbot, Michael Peake, Timothy Perren, Charles Wilson, David Dodwell, published August 31, 2016. Interestingly, there is nothing in the study that explicitly states that half, or 50%, of cancer patients are killed by chemotherapy. Rather, the authors state: This study shows that the SACT [Systemic Anti-Cancer Therapy] dataset provides insight into the factors affecting early mortality of patients in England. It suggests that treatment intent (curative or palliative), age, performance status, whether patients had received SACT before the qualifying treatment used for this study, and sex and stage (lung cancer only) all affect the 30-day mortality risk. The discrepancies between patient categories for each of these factors point to opportunities for improvements in care. The identification of hospitals with significantly higher 30-day mortality rates will promote review of clinical decision making in these hospitals. The findings presented here could be used to improve clinical outcomes. Note that the study suggests treatment intent. And that the findings could be used to improve outcomes. The use of such words imply that the study is non-conclusive and further studies need to be made. In regard to chemo, the study states: Although we identified several factors affecting 30-day mortality risk, our population-based dataset included only patients that received SACT, so we cannot confirm whether patients would have had better outcomes if they had not received SACT. Similarly we cannot assess whether patients who did not receive SACT might have benefited from treatment. Our data also suggest that 30-day mortality might be higher than previously estimated by several clinical trials. The 30-day mortality rate after SACT with curative intent for NSCLC reported here is high at 3% compared with published trial data for the standard treatments, which suggested that 0·8% of patients died from treatment-induced toxicity when chemotherapy was given as adjuvant treatment alongside surgery. These patients have been assessed as fit enough for radical curative treatment (eg, thoracic surgery with adjuvant systemic anticancer therapy), estimated to increase the average NSCLC 5-year survival by 4–5%, as reviewed by Heon and Johnson.28 Therefore, the high mortality rate we report here is a concern because it could reduce any benefit from this intervention. It amazes me how alt-med spin doctors conjure misconceptions from facts. And, sadly, FB armchair oncologists, with their knee-jerk reactions, re-post alt-med’s false claims as if they were scientific proof. In doing so, they help feed the fears of cancer patients who are dealing with a life-threatening disease. After all, why take a treatment if it has a 50% chance of killing you? The critical problem is that most people - in particular, people who don’t have cancer - are not educated about the nature of chemotherapy. If they were, they would know that chemo isn’t about curing cancer. It never has been. Chemo is about giving a terminal patient another day, another week, another month. Chemo is about shrinking cancer cells before surgery. Chemo is about killing cancer cells after surgery. Chemo is about killing cancer cells that have re-invaded a patient’s body. There is no doubt about it - chemo is powerful. It has a multitude of side effects; its debilitating after effects can last for years. It may or may not send cancer into remission. Its efficacy is dependent on several factors including one’s age, health conditions, and immune system. There are no guarantees. I know from personal experience the effects and lingering after effects of chemo. I went through 16 hard rounds of chemo - four rounds of neoadjuvant chemo with a regimen of Oxaliplatin (Eloxatin) and Capecitabine (Xeloda) and twelve rounds of adjuvant chemo with a regimen of Irinotecan (Camptosar). I went through total hair loss, fatigue, nausea, diarrhea, loss of appetite, weight loss, cold sensitivity, peripheral neuropathy. Some of those remain issues that I deal with today long after my chemo regimen ended. Despite the difficulties, I have never once regretted taking chemo. As of this writing, I have been NED for 19 months. And chemo has played a crucial role in preventing my cancer from metastasizing. And I’m not alone. There are countless other survivors who will attest to the fact that they are alive because of chemo. However, alt-med proponents and FB armchair oncologists would rather ignore the inconvenient truth about chemo. The main danger is the impact that such misinformation has on newly diagnosed cancer patients. They may decide to refuse treatment based on the falsity of alt-med's claims. Certainly, cancer patients have the right to decide whether they want chemo. But their decision should be based reliable information rather than the misinformation disseminated by alt-med proponents and FB armchair oncologists. Armchair oncologists, in particular, may think they are helping to save people when, in fact, they may be sending them to an early, agonizing death.
© Robert DesJarlait, 2018 I’m tired. I’m weary. When I say I’m weary, I don’t mean physically. I’m weary emotionally and spiritually. It isn’t a constant weariness. It comes and goes. It comes especially when I receive news of someone I know who has contracted cancer. This past summer alone, I personally know of six people who have contracted cancer. These are close and dear friends, people who are known in our community. These are people who have been newly diagnosed. In some cases, the cancer is untreatable and, hence, terminal. In addition to that, several people I know are batting recurrence through treatment. And then there are the people I don’t know personally but know through Facebook. People who have contracted cancer, people who have died from cancer, and people who have lost loved ones to cancer. Why all this cancer in our community? I don’t know. However, I’m not really thinking about the reasons for the rates of cancer among my friends. I’m thinking about those who are getting this horrid disease. It’s unending. And I may be more attuned to this depressing news because I’m always writing about it. It brings up the question - why them, not me? I don’t know. Perhaps I’m here to tell the story. Is it normal to feel this way? I thought maybe it was just me. But then I went online and found several articles on cancer survivor’s guilt. As it turns out, the way I feel at times like this is fairly common among cancer survivors. And the feeling is - some have survived, others haven’t. With it there can be a sense of guilt. I’ve survived, you haven’t. I don’t say that with any pride or self-indulgence. Rather I say it with tears and sadness. Survivor’s guilt is part of the psychological effects that impact survivors. Those effects include fear of relapse or death, chronic anxiety, uncertain future, fear of dependency, PTSD or depression, and survivor’s guilt. People, including caregivers, are generally unaware of the inner feelings that survivors deal with. If a loved one is surviving cancer and living in partial or complete remission, then they assume that the person is okay. But they don’t really see what’s under the surface. And that’s why being a survivor is a private, and oftentimes, isolated experience. You can’t know what it’s like being a survivor unless you are a survivor. Certainly, those psychological impacts are part of the reason why I write and talk about cancer. In turn, I have my critics. Some people, especially elders, have told me that I shouldn’t talk about cancer. For them, the word is a stigma. Apparently, if you don’t talk about it you won’t get cancer. Then there are others who have told me to “get over it.” Get over what? Get over cancer? I wish I could. But I’m stuck with it for the rest of my life. And, for me at least, this is where a few of those psychological factors come into play, especially fear of relapse and uncertain future. My cancer, or more specifically my recurrence cancer, has been in complete remission for over 18 months. That doesn’t mean that I’ve been cured of cancer. Only when I’ve been in complete remission for five years can I be considered to be cancer free. I still have 3 1/2½ years to reach that goal line. And, as defined by the American Cancer Society, “A complete response or complete remission does not mean the cancer has been cured, only that it can no longer be seen on tests.” The notion that cancer unseen but lurking in my body creates the thought that it could return. Maybe not today but what of tomorrow? That’s not to say that I live in fear. But I’m not fearless. Perhaps the best way I can put it is that I have a fearful respect toward my cancer. As Augustus Waters says in The Fault in Our Stars: “And what is my cancer? My cancer is me. The tumors are made of me. They're made of me as surely as my brain and my heart is made of me.” I can’t say that I’m not subject to psychological factors. I am. But I’m not overwhelmed by them. Just as cancer is a part of me, so too the psychological factors. Survivor’s guilt is probably the one I deal with the most. But then, that is the factor that I’m most exposed to because of the news I receive on social media. And what strikes me the deepest are friends who are diagnosed with late Stage IV terminal cancer. In the blink of an eye, their world has changed in which there is no tomorrow. They haven’t the opportunity to become survivors. As Augustus Waters says, cancer is a civil war with a predetermined winner. For some, the civil war is lost before even stepping onto the field of battle. Of course, life goes on. I have to continue what I do and live the life I have. And tell the story. © Robert DesJarlait, 2018
Stories are told in different ways. Some stories are told by words that are written or spoken. Other stories are told through pictures. Some stories are told with both words and pictures. Cell phones have, of course, changed the way we tell stories through the photographs we take. The Kodak moment has become the smart phone moment. We no longer have to carry the extra baggage of a camera with accessories. Rather, we carry our camera in our pocket. When we buy a smart phone, we more often than not do so for a camera that allows us to take good, quality photographs that document our personal lives and our relationships with others. On the internet and social media, we download our photos and post them with text. We become storytellers by proxy although it is the photos that emphasize our experiences. With that said, I didn’t really photograph my experiences in Cancerland in the beginning. The only photo I remember taking was from my bed in the cancer ward at U of M/Fairview hospital. The view outside my window was the Mississippi River. Riverside Park was across the river. In the summers of my young boyhood, my family picnicked there on Sunday afternoons. We only lived a few blocks away in the Seven Corners area. Although I posted the photo on Facebook with a short narrative, the post and the photo got lost. Hence, the phase of my cancer journey that I call Stage I was largely documented by others, most notably by Ivy Vainio. Ivy is a preeminent photographer whose photos have been featured in exhibitions and articles. She is something like my personal “paparazzo” who has literally taken hundreds of photographs of me. I don’t know why I am one of her favorite photo subjects, but Ivy has essentially photo-documented my life from 2012 to the present-day. Ivy’s photos from 2013-2015 (Stage I), along with several others, document my life albeit my life lived as a cancer survivor. Things may appear normal but under the surface I was going through a healing period. Whether I was at a powwow or in a march, my physical capacity was limited as a result of my colon cancer surgery in May 2013. The second phase of my cancer journey, that I call Stage IV, begin with photographs that I took of my experiences in the deeper world of Cancerland - a world of CT and PET scans, chemotherapy, biopsies - and my reactions of what I was going through. My goal wasn't to photograph everything but enough to leave a record to tell my story. This then is my cancer journey as told through photographs and words. From the moment that it began to the present. However, there is no ending because the cancer path goes ever on. Stage I 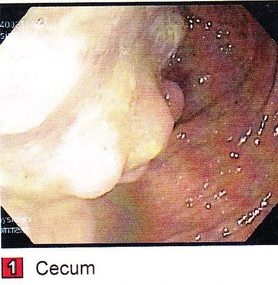 My cancer journey began on 4/26/2013 with a colonoscopy performed by Mohamed A. Hassan, MD, at the University of Minnesota Medical Center, Fairview, Endoscopy Department. The colonoscopy was ordered by Genevieve B. Melton-Meaux, MD, gastroenterologist/surgeon, to whom I was referred to by my doctor, Katherine B. Bickel, CNP, at the Native American Community Clinic. As noted in the colonoscopy report - Impression: Malignant partially obstructing tumor cecum. So began my battle with The Beast. Five days later, I underwent my first CT scan. Examination: CT Chest, Abdomen and Pelvis 5/1/13 Indication: Right-sided colon mass. IMPRESSION 1. Lobulated mass involving the distal cecum and ascending colon consistent with known colon carcinoma. There is intussusception tip cephalad, this is then drawn is a normal, nonobstructive, appendix more cephalad as well. The terminal ileum is somewhat thickened. It may well be that the terminal ileum is thickened because of intermittent intussusception. The size of the mass is likely accentuated due to intussusception. There are multiple lymph nodes in the medial mesentery to a sending colon. The size and number are worrisome for possible metastatic involvement. 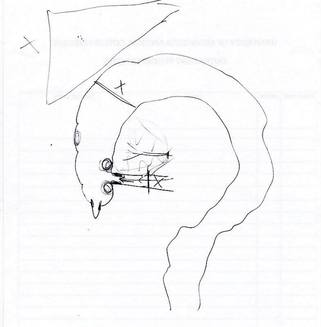 Following my colonoscopy and CT scan, I met with Dr. Melton-Meaux to discuss my surgery. Dr. Melton-Meaux did a drawing of the tumor in my ascending colon. The triangular shape is my liver. She explained that the section of my colon marked by the X would be removed. On 5/14, Dr. Melton-Meaux performed laparoscopic surgery to remove the tumor. My cancer was classified as Stage I. As such, chemo wasn't required. The tumor hadn't broken through the wall of my colon and into my lymph nodes. However, I was put on a high-risk colon cancer surveillance program that included annual colonoscopies and CT scans for five years. I felt that I had dodged a bullet. The five-year survival rate for Stage I colon cancer patients is 93%. I couldn't ask for betters odds. I had beat The Beast in my first battle. My CT scans for 2014 and 2015 reaffirmed the survival stats. I was NED (No Evidence of Disease). Although polyps were found in my post-surgery colonoscopies, none were precancerous (that is, not until 2016). My main concern was an incisional hernia that had developed. However, Dr. Melton-Meaux or Dr. Greeno, my oncologist, didn't feel it was an issue at this point. CT 5/27/14 IMPRESSION 1. Postsurgical changes of a right hemicolectomy with resection of the previously seen cecal mass. No evidence of metastatic disease in the abdomen or pelvis. 5. New incisional hernia containing nondilated loops of small bowel.  Kiwenz Ojibwe Language Camp, 2014 / Photo by Ivy Vainio Following my surgery, my perspective of life and priorities changed. My body, mind, and spirit had been through a traumatic experience. Healing takes time. As part of my healing, I continued to be engaged in various cultural and environmental activities. I began to advocate about cancer in the Native American community. I started a blog to provide insights about Cancerland. Regardless of what I was doing, cancer was part of my renewed persona.   Being a cancer survivor brings many gifts, both material and spiritual. The gifting of my cancer medallion in 2014 was one such gift. The beaded medallion was made by Naakiiyaa Wilson and gifted to me by Ivy Vainio. The ribbon represents the blue ribbon for colon cancer. It encircles a dragonfly, one of my favorite insects.  Photo / Ivy Vainio  Photo / Ivy Vainio  Photo / WCCO News The People's March in November 2014 proved to be a test of my physical stamina. The march was one of two marches held concurrently to protest against the Washington Redskins name and mascot. (The other march was organized by National Coalition Against Racism in Sports and Media.) The People's March was organized by several Twin City grassroots organizations. We brought 1400+ marchers to the streets. I could only make it halfway before handing my eagle staff to my friend Patrick Shannon-Skildum to bring it home to the stadium.  Powwow for Hope, May 2015. Photo / Ivy Vainio My path as a cancer survivor is entwined with the American Indian Cancer Foundation's annual Powwow for Hope (PFH). In 2013, I attended my first PFH. My intention was to dance for my father, Patrick Robert DesJarlait, who died from stomach cancer in 1972. Ironically, by the time that this powwow came up on my calendar, I was dealing with my own cancer.  Photo / Patricia Shepard  Photo / David Goodner Tar Sands Resistance March, June 2015. On a hot, sweltering day in St. Paul, over 5,000 of us marched to the Minnesota State Capitol to bring our message - no more tar sands, no more Enbridge. This was a magnificent march and incredible experience. I only made it halfway with my eagle staff. I handed it off to another individual who brought it to the steps of the capitol.  Manidoo-giizhikens (Little Cedar Spirit Tree), Grand Portage, 2015. Photo / Ivy Vainio. Like many other Anishinaabe people, Manidoo-giizhikens was a tree that I was familiar with through stories and photos. I never expected to see it, let alone stand next to it, touch it, and place asemaa (tobacco) under it. This was undoubtedly an integral part of my healing journey. This is one photograph of several from a photo shoot with Ivy.  Screen capture, NFL Films  Photo / Miziway Migizi DesJarlait Minnesota Vikings Native American Heritage Month celebration, November 2015. A life-long Minnesota Vikings fan couldn't ask for much more than this - dancing before a home crowd of 54,000 at halftime and getting a ringside seat to the Vikings vs. Packers game. The video, shot by NFL Films, has been viewed by over one million online viewers.  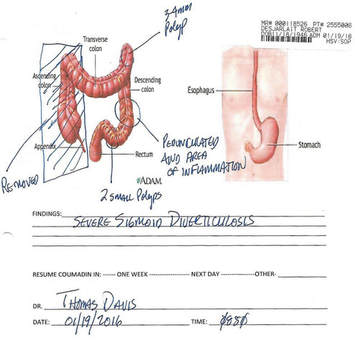 The year 2016 began with a ominous reminder. After a delay of six months, I finally had a colonoscopy performed at the Mille Lacs Health System. Three polyps were found and removed. The 3-4mm polyp in my Traverse colon was confirmed by biopsy to be precancerous. This didn't mean that cancer had developed again in my colon; rather, the precancerous polyp signaled the conditions, in time, for cancer to develop. Of course, it bothered me that cancer, in any shape or form, had been in my body. It raised the question of whether I would ever really be cancer free. Stage IV    On June 23, 2016, I had appointments for lab/blood work, CT scan, and a meeting with my oncologist, Dr. Edward W. Greeno. Because of the early morning appointments, my wife and I stayed at the American Cancer Society Hope Lodge. Little did I know what the day would bring.   After lab work, I did my CT scan. We had to wait two hours before we could see Dr. Greeno and get the results of the scan. The first words that Dr. Greeno said to me was: "Well, Robert, we found something on your scan." I was crestfallen. He explained that a spot was found on the left lobe of my liver. In the photo, my liver is on the left and the left lobe near the top. The dark spot is clearly visible. We were both surprised since we were aware of the outstanding stats for Stage I survival rates. I was no longer Stage I but now Stage IV because cancer cells had traveled through my blood stream and had metastasized to my liver. Dr. Greeno wanted to be sure that the cancer hadn't spread elsewhere, so he ordered a PET scan for the next day. CT 5/23/16 IMPRESSION: 1. New hypodense cystic-appearing lesion in the left hepatic lobe, measuring up to 2.4 cm, most compatible with metastases in this patient with a history of cecal adenocarcinoma.  The PET can confirmed the results of the CT scan - colon cancer mets to my liver. But there was a new concern. A lymph node my neck - the deep cervical lymph node - near the bottom of my neck and collarbone lit up. It would be extremely unusual for cancer cells to travel and metastasize in an area so distant from my cancer's point of origin. But the only way to find out was to perform a biopsy of the lymph node. PET Oncology Whole Body 5/24/16 IMPRESSION: 1. In this patient with a history of cecal adenocarcinoma status post resection, there is hypermetabolism at the periphery of the new hepatic segment 3 lesion, consistent with metastatic disease. 2. Markedly hypermetabolic cervical lymph nodes bilaterally are nonspecific. While this would be atypical for metastatic colon cancer, malignancy cannot be excluded and biopsy should be considered for further evaluation.   A fine needle aspiration biopsy was performed on 6/10. Seven days later I received the results of the biopsy: “salivary gland neoplasm, morphologically consistent with Warthin's Tumor which is a benign cystic tumor of the salivary glands containing abundant lymphocytes and germinal centers.” So, I had a tumor in my neck that was benign with a 3% chance of becoming malignant in 20 years. It was a risky operation. Nerves to the face located next to the lymph node could be severed and cause paralysis of the right side of my face. As a result, it was decided that the Warthin's Tumor would be left alone and not surgically removed.  On the way home from my lymph node biopsy, we stopped at the Relay for Life event at Mora (MN) that I had previously signed up for. I was stressed out, tired, and sore, and not interested in participating in the survivor's walk. I just wanted my survivor t-shirt. We tried to find my luminaria bag but there was simply too many that lined the Mora Fair Grounds. Given the overwhelming number of luminaria, it was obvious that cancer had deeply impacted this small farming community.       In July 2016, I had my first infusion of neoadjuvant chemo. I was scheduled for six rounds of Oxaliplatin via IV and daily tabs of Capecitabine. The chemo was intended to shrink the cancer on my liver. I had a mild reaction to the third round of Oxaliplatin and a severe reaction to the fourth round. As a result, the remaining chemo infusions were cancelled.    It didn't take long for the chemo side effects to take hold. The most immediate was the cold-sensitivity effect. Anything touched by my bare feet and hands resulted in a numbing, tingling sensation. I had to use rubber gloves when using metal utensils and getting things from the refrigerator. I had to drink through straws. My palate changed; some food lost its flavor and other foods were overly intense with flavor. To make up for needed vitamins and minerals, I drank a daily smoothie with fruits and vegetables with Muscle Milk Protein powder. The "What To Eat" book helped me to make more nutritious meals. "The Cancer Survivor's Companion" helped me deal with emotional issues. "Mindfulness-Based Cancer Recovery" enabled me to calm my mind and deal with less stress. I also maintained traditional practices - smudging myself with sage and sweet grass, smoking my pipe, and offering asemaa (tobacco) in the mornings.  In July, I met with Dr. Michele Montejo Loor, MD. By this time, my incisional hernia had grown quite large. The hernia had been noted in previous CT scans and PET scan. Because of its size, it was decided that it would be removed during my liver surgery. I also met with Dr. Eric Jensen, the Surgical Oncologist who would be performing my liver surgery. Surgery was scheduled for November (2016). I would be undergoing two surgeries in one shot - one for the liver and one for the hernia.   In August 2016, a port was inserted for easier access for chemo infusion and for lab/blood work.      Photo / Francisca Wiyakaluta Folkestad  One of the side effects of my chemo was hair loss. I wasn't losing my head hair per se; rather, my hair was coming out in clumps. I also lost my eyelashes. My mustache and goatee remained untouched. On the morning of my port insertion, I had Nan cut off my pony-tail and scalp-lock. The following day, I went to a barber and had my head shaved bald. I kept my pony-tail and scalp-lock, but a week later I took the rest of my hair, made a medicine bundle, and released it on the Mississippi River. A pre-surgery CT scan was performed in October. The cancer was growing albeit slight. The hernia received special attention since it would be part of the surgery that would be performed. CT 10/7/16 IMPRESSION: 1. Slight increased size of left hepatic metastasis. HISTORY: Metastatic colon cancer, assess response to treatment.Malignant neoplasm of colon, unspecified. Secondary malignant neoplasm of liver and intrahepatic bile duct. FINDINGS: There is a tiny fat-containing left ventral abdominal wall hernia (image 77 series 2) with an opening measuring approximately 0.9 cm. Tiny fat-containing umbilical hernia (image 75 series 2) is also noted with an opening measuring approximately 0.6 cm. There is a moderate to large ventral colon and small bowel containing hernia with an opening measuring 5.6 cm. No evidence for incarceration or strangulation of bowel is identified. No bowel obstruction is seen. This hernia was also seen previously.  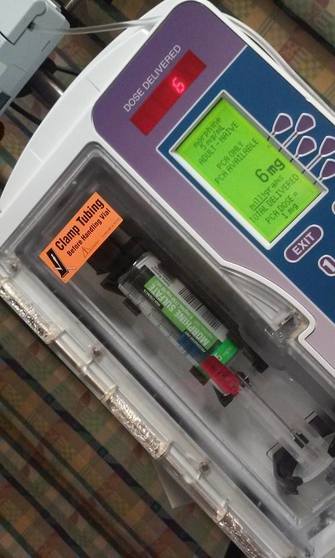   On November 10, 2013, I underwent surgery to remove the left lobe of my liver and to repair my incisional hernia. I was in OR for 9 hours - three hours for the liver and six hours for the hernia. There is no greater joy than waking up and seeing your family at the end of your bed. Originally, the surgery was going to be laparoscopic, but Dr. Jensen, the head surgeon, decided that open surgery was the best way to get at the liver and hernia. Needless to say, I was in a lot of pain and made ample use of my morphine pump. Nan was by my side for nearly the four full days that I was in the hospital. My eagle fan, that I hung from my IV stand, provided me with spiritual protection and nourishment. The operation left me with a 9” incision. Twenty-five staples were used to close it. The best news came from Dr. Jensen. He said I was clean - no other cancer was found on my organs. Once I got home, Nan assumed a strong role as my caregiver. I had a drainage tube attached and Nan had to empty it daily and record how much fluid was collected in the discharge cup. I was also given 28 day supply of Enoxaparin syringes. These were used to prevent deep vein thrombosis prophylaxis to prevent blood clots in the lower leg and thigh. Nan provided me with my daily injections. 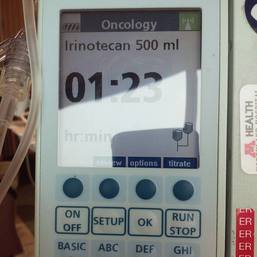 In January 2017, my new cancer regimen included 12 rounds of adjuvant chemo and a high-intensity surveillance program - CT scans every three months for two years followed by two CT scans a year for three years and annual colonoscopies. The Irinotecan chemo was a rugged chemo with side effects that included nausea, vomiting, diarrhea, fatigue, loss of appetite. My hair had been growing back following the cessation of neoadjuvant chemo that was given prior to my surgery. Once I began Irinotecan, my hair turned brittle and began to fall out. I basically suffered total hair loss - loss of head, facial, and body hair.    In 2017, I appeared in the booklet "Cancer Plan Minnesota 2025" by the Minnesota Cancer Alliance, and colon cancer promotional material for the American Indian Cancer Foundation. I was featured in publications and articles including "A Community Effort," Cancer Today Magazine (2014); "Meet One Million Strong," Fight Colon Cancer (2014);"Poor Cancer Care for Native Americans Might be a Treaty Violation," Newsweek Magazine (2016). I became a contributing writer at I Had Cancer. My articles include "Cancer is Never Really Out of Sight, Out of Mind" (2017) and "We Are Lanterns In The Darkest Night" (2018). I was also featured on the cover of Mazina'igan (2018), a publication by the Great Lakes Indian Fish & Wildlife Commission.      Powwow for Hope photos / Ivy Vainio In May 2017, my wife/caregiver and I gifted the American Indian Cancer Foundation (AICAF) with an eagle staff at their 6th Annual Powwow for Hope. The eagle staff was created by Nan and I from a dream vision that I had. In turn, I was gifted with a beautiful walking staff. Nan was honored at the Caregiver's Honor Dance and received the blanket "Renewal" by Sarah Agton Howes.   Lake Vermilion Powwow. Photo / Ivy Vainio In April 2018, I became the spokesperson for the Colon Cancer Powwow Initiative. The initiative was sponsored by the American Indian Cancer Foundation through a grant by the Minnesota Health Department. From April to June, we visited six powwows - Osseo Indian Education Powwow, Augsburg Powwow, U of M Indian Students Powwow, Leech Lake Powwow, White Earth Powwow, and Lake Vermilion Powwow. The main focus of the initiative was to tell my survivor story and create awareness about colon cancer, and cancer in general, in Indian Country.  Photo / Stephanie Thompson My main support group is my family - my wife, Nan, daughters, Meeg-wun Giizhig'kwe, Makina Anung'kwe, sons, Miskwa Mukwa and Miziway Migizi, and my grandson, Tae-Tae. But there are many others - extended family members, dear, close friends, and many, many others who I haven't met and may never meet. Without them, my cancer journey would not be possible.  Photo by Ivy Vainio The story doesn't end here. There will be chapters to add in the days and months - and hopefully, years - ahead. New words and photos will unfold. However, being a Stage IV cancer survivor doesn't allow me to look too far into the future. Despite the lingering after-effects and the ensuing cancer PTSD, my lab/blood work show my immune system and organs to be in fairly good shape. The best news is that I've been cancer free for over 18 months. My CT scans since November 2017 have consistently declared NED (No Evidence of Disease): IMPRESSION: 2. Postop changes status post partial hepatic and colon resection are again noted. No new evidence for metastasis or recurrent malignancy is seen. In the meantime I'll continue to tell and live my story until I'm called homeward to the Land of Everlasting Happiness. Until then, I will appreciate each day that is given to me. May the Creator bless you and yours. Mii'gwech.  Photo / Patty Maquire We Are Lanterns In The Darkest Night Whose flames illuminate tales Of paths trodden in the past And of paths to tred yet ahead; Wind nor rain Shall extinguish our light For our stories Will be forever told In the hearts and minds Of those we leave behind.  Photo / Steve Premo Postscript: Chi-mii'gwech to Ivy Vainio for the literally hundreds of photographs that she has taken of me since 2012. The majority of photos in this article, other than mine, were taken by Ivy. Ivy and her husband, Dr. Arne Vainio, are dear friends who have been two of my strongest supporters on my cancer journey. Kiitos to both of you. © All Rights Reserved, 2018, Robert DesJarlait All photos except where noted by the author and may not be used without written permission © 2018, Photos, Ivy Vainio Medical record excerpts and diagrams property of the author. For reproduction information, contact the author at [email protected] 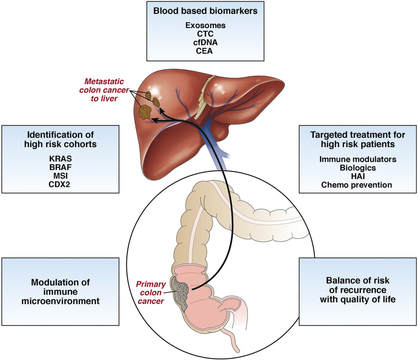 I found out this morning that my cancer is Stage IV. After talking to other survivors and doing my research at reputable cancer sites, I found that my recurrence in 2016 has uncomfortably moved me into the Stage IV category. "If the cancer has spread to distant parts of the body, it is called metastatic recurrence. Metastatic cancer is also called stage 4" (Anne Schott, associate professor of medical oncology at the University of Michigan Rogel Cancer Center). In my case, when my colon cancer spread to the left lobe of my liver, I moved into the Stage IV category. The metastasis didn't occur via my lymph nodes because those were removed when my ascending colon was removed. Rather, the invading cancer cells traveled through my blood stream and established a colony on the left lobe of my liver. It's estimated that should recurrence occur, it usually reappears in the third year following surgery. That is exactly what happened to me. The photo that I included provides a graphic look at colon cancer metastasis to the liver. For the uninformed, there are four stages in cancer:
When I first contracted cancer in 2013, my ascending colon was removed. After the tumor was biopsied, it was classified as Stage I because the cancer hadn’t spread beyond the walls of my colon into the lymph nodes or other parts of my body. As such, chemo wasn’t required. Thereafter, I was placed on a low-intensity surveillance program – CT scans once a year for five years. Why five years? Because the 5-year survival rate for Stage I colon cancer patients is 93%. If you remain NED (No Evidence of Disease) in the five-year timeline, you are then considered free of cancer. For the first two years, I was NED. But in the third year, 2016, my CT scan revealed colon cancer metastasis to the left lobe of my liver. I went through four rounds of neoadjuvant chemo, i.e., chemo before surgery, and twelve rounds of adjuvant chemo following surgery. I was placed on a high-intensity surveillance schedule – CT scans every three months for three years, followed by two CT scans a year for two years. At the present writing, I’ve had seven scans and remain NED. Through all this, I was totally unaware that my status as a cancer patient had changed. I knew I was a high-risk cancer patient, but I didn’t know that in Cancerland parlance, I was a Stage IV survivor. Why didn’t I know? Because I didn’t ask. It’s important to dialogue with your oncologist. I didn’t do my research to have a better understanding of high-intensity surveillance. Had I done so, I could have asked when my oncologist asked me if I had any questions. When it comes to cancer, a patient needs to have an understanding of the type of cancer that they are dealing with, an understanding that enables them to ask questions when talking to their doctor. In my case, I dropped the ball and found out later than sooner. Stage IV almost sounds like a death sentence because “metastatic cancer is rarely curable. Cancer, by its very nature, is designed to spread. Cancer develops when your body's cells go awry and begin reproducing and invading surrounding tissue in a way that nature did not intend. The cancer cells travel to different parts of the body and begin forming new tumors…The goal for treating a spread cancer is to reduce tumor size and relieve some of the symptoms that patients experience. This allows us to prolong an individual's life and, in many cases, allows a person to live a high-quality life” (Anne Schott). And therein is the hope – the hope for a high-quality life despite dealing with metastatic cancer. But with it comes the necessities at looking at my priorities. There are a few things I want to accomplish. So I need to focus on those. Don’t get me wrong. I’m still a long way from journeying to the Land of Everlasting Happiness. But when the specter of death is lurking nearby, there are things you want to get done. As I’ve said before – the cancer journey goes ever on. There are many twists, turns, and tangents on this path. And today, I’ve wandered onto a new tangent. © Robert DesJarlait, 2018
 The American Indian Cancer Foundation eagle staff at Lake Vermilion, primed and ready for Grand Entry. Endaso-Giizhik Ojibwemong Makwa Nindoodem Miskwaagamiiwi-zaaga’iganiing indoojibaa Niin amogo-ishkwanidiwin (My Ojibwe Spirit Name is Everyday I belong to the Bear Clan, I am from Red Lake I am a cancer survivor.) This was usually the way I introduced myself in my speeches for the Powwow Colon Cancer Initiative. The initiative was a project that was sponsored by the American Indian Cancer Foundation (AICAF) with a grant from the Minnesota Department of Health. Six powwows were selected to bring a message of hope and awareness in regard to colon cancer. The initiative began in April and ended on the weekend of June 22-24 at the Lake Vermilion Traditional Powwow located on the Bois Forte Ojibwe Reservation in northern Minnesota along the U.S and Canadian border. The people who lived in the region were called Bois Forte (Strong Wood) by the French. This was based on the name that the people called themselves - Zagaakwaandagowininiwag (Men of the Thick Fir-woods). One place of habitation was Onamni – Lake of the Sunset Glow. It was later translated by the French as Lake Vermilion. Lake Vermilion was established by the treaty of 1854. Nett Lake and Deer Creek were established by a treaty in 1866. All three comprise the Bois Forte Band of Ojibwe. It was my first time at the Lake Vermilion powwow. Somewhat surprising considering that I’ve been dancing for about 35 years, traveling all over Ojibwe country for powwows, but never attended this one. I know the reason why. In previous years, I would have attended the powwow as a dancer. But Gichi-Manidoo (the Creator) moves in mysterious ways and I wouldn’t go to Lake Vermilion until it was meant to happen. My role as an amogo-genawenimaad (cancer advocate) in Indian Country has taken me to places where I’ve never been before to bring a message that, I believe, is a mandate from Gichi-Manidoo. Lake Vermilion was one such place. I brought the AICAF eagle staff with me. This was the third powwow of the initiative that the eagle staff was part of the Grand Entry procession. The eagle staff was made by me and Nan, my wife and caregiver. It was created from a dream vision that I had and was gifted in 2017 to AICAF at the Powwow for Hope. The powwow began on Saturday afternoon. Surprisingly, I was the only one with an eagle staff. (Two Bois Forte eagle staffs would join the Grand Entry for the Saturday evening and Sunday sessions.) Although eagle staffs aren’t necessarily required to begin Grand Entry, their presence brings balance and meaning to a powwow. To me, it was significant that the AICAF eagle staff would open the powwow. It had center stage. It provided the opportunity for the spectators to see this beautiful, and meaningful, eagle staff lead the color guard and dancers into the dance arena.  Lining up for the afternoon Grand Entry at Lake Vermilion.  Saturday afternoon Grand Entry at Lake Vermilion. Later in the day, I gave my speech. I began this one differently. Rather than beginning with my experiences as a amogo-ishkwanidiwin (cancer survivor), I talked first about the eagle staff. I spoke about the meaning of the feathers and the colors on the staff and that the staff represented those we have lost to cancer, the survivors, and the caregivers. I then spoke about my experiences as a survivor, the effect of cancer in the Native community, and the importance of getting screenings.  Giving my speech at Lake Vermilion. Following my speech, a woman came up to me, introduced herself as a cancer survivor, thanked me for speaking for survivors, and shared her story. Her name was Christina Primo-Hujanen. On a Facebook post, she was asked about the nature of our conversation. Christina responded: “Because we are both cancer survivors and he and I were talking about how it affects us but people don't like talking about it and people don't realize the after effects and how people don't understand the traumatic after affects. Remission means it comes back. Just don't know when.” Cancer survivors share a special bond. We are a band of brothers and sisters engaged in a different kind of war. Christina is one of several survivors that I’ve met at various venues that I’ve been to and who have shared their stories with me. It’s people like Christina that make my work worthwhile.  One survivor to another. With Christina Premo-Hujanen. I’m grateful for the opportunity that the Powwow Colon Cancer Initiative has provided me with. Hopefully, my words will motivate others to become familiar with symptoms and get screenings. And although the initiative has ended, my work continues. The Journey goes ever on.  On the Lake of the Sunset Glow. © Robert DesJarlait, 2018
All photos by Ivy Vainio © Ivy Vainio, 2018  Caregiver Honor Dance for Nan, 2017 Powwow for Hope, Photo by Ivy Vainio Sometimes I get these odd thoughts early in the morning as I sip my coffee. This morning was a "what-if" thought. What if I had cancer but Nan and I weren't together? If the circumstances were different, would I be an advocate, writer, and blogger of cancer in the Native community today? Probably not. I would most likely be bitter, angry, and depressed. I know that I wouldn't be able to deal with The Beast alone. Over the years (and it's odd to say "years," but I've been on this journey for over six years now), in the cancer wards and clinics that I've been to, I've seen those who are alone. They have no one to accompany them to give them loving support. I've seen the pain, suffering, and depression etched on their faces. Like a conduit, I absorb all that. It strikes me deep within. It becomes the residue of memories and experiences that I’ve had in Cancerland. Memories of the dark, lonely hours in the cancer ward while the patient next to me suffers in silence because there are no loved ones to visit him. In the cancer clinics, people who suffer silently waiting to see their oncologist as they sit alone without loved ones accompanying them. Many of these people have spouses and partners who have abandoned them which deepens their pain. But then there are those who have someone with them and it’s like going from dark to light. They are more comfortable and a bit more relaxed because they are not alone in the darkness that filters through their lives. Their situation is more acceptable because they have someone next to them that usually includes their spouse/partner - and a support group of offspring, siblings or friends. In my language we call them Gaatiniwekweg (female caregivers) or Gaatiniwewininiwag (male caregivers). They play an essential role in our health and well-being. They are there to get us to our appointments. They are there to listen to our diagnosis. They are there to listen to our complaints and our fears. They are there to give us encouragement. But most of all, they are there to give us their unconditional love. Not everyone has one. And without one, the journey can be extremely difficult. Certainly, some people can get through it alone, but for others, it can be an emotional struggle. I’m grateful that I have one. One who has been with me every step of my journey. I know it hasn’t been easy for her. The stress and anxiety of a yet unknown future affects her. But she has never wavered from being my support system during these often difficult times. So, my “what if” moment has turned from what could have been to what it is not. My Gaatiniwekwe has shown me that life has meaning in the darkness of night. © All Rights Reserved, Robert DesJarlait, 2018
|

Robert Desjarlait
|
 RSS Feed
RSS Feed
